You might also like
- UNIT 4 - New Challenges: Urja JoshiDocument72 pagesUNIT 4 - New Challenges: Urja JoshiRadhey RavalNo ratings yet
- Presented By:-Pallavi Chawla Pallavi Dhiman (BDS - 3 Year)Document28 pagesPresented By:-Pallavi Chawla Pallavi Dhiman (BDS - 3 Year)tinu989No ratings yet
- AIDS in The PhilippinesDocument29 pagesAIDS in The Philippinesjaninasuzette100% (1)
- HivDocument29 pagesHivSUTHAN100% (2)
- Hiv Infection and AidsDocument51 pagesHiv Infection and Aidspokhara gharipatanNo ratings yet
- Human Immunodeficiency Virus (Hiv)Document52 pagesHuman Immunodeficiency Virus (Hiv)AswinNo ratings yet
- Nursing Clients With HIV Infection and AIDS: Learning ObjectivesDocument11 pagesNursing Clients With HIV Infection and AIDS: Learning Objectivesmorynayim-1No ratings yet
- Immune Deficinecy: By: Kirk Odrey O. Jimenez R.NDocument51 pagesImmune Deficinecy: By: Kirk Odrey O. Jimenez R.NKirk08No ratings yet
- HIV Structure, Symptoms, Transmission, Diagnosis and TreatmentDocument28 pagesHIV Structure, Symptoms, Transmission, Diagnosis and TreatmentAlex SamNo ratings yet
- Is HivDocument50 pagesIs HivRodriguez, Jhe-ann M.No ratings yet
- Delfin, RMTDocument34 pagesDelfin, RMTAffie SaikolNo ratings yet
- Acquired Immune Deficiency Syndrome or Acquired Immunodeficiency SyndromeDocument37 pagesAcquired Immune Deficiency Syndrome or Acquired Immunodeficiency SyndromeSumon ChowdhuryNo ratings yet
- Human Immunodeficiency Virus (Hiv)Document30 pagesHuman Immunodeficiency Virus (Hiv)Manesa ManeshaNo ratings yet
- Human Immunodeficiency VirusDocument24 pagesHuman Immunodeficiency VirusMalueth AnguiNo ratings yet
- DR - Dr.efrida Warganegara, M.Kes., SP - MKDocument30 pagesDR - Dr.efrida Warganegara, M.Kes., SP - MKDedy SantosoNo ratings yet
- Nursing Clients With HIV Infection and AIDS: Learning ObjectivesDocument11 pagesNursing Clients With HIV Infection and AIDS: Learning Objectivesmorynayim-1No ratings yet
- Dr. G. Thiruvenkadam Post Graduate Dept of Pediatric & Preventive DentistryDocument31 pagesDr. G. Thiruvenkadam Post Graduate Dept of Pediatric & Preventive Dentistryதிருவேங்கடம் கோபாலன்No ratings yet
- SEMINAR-Clinical Microbiology: Topic-Human Immuno-Deficiency Virus (HIV)Document54 pagesSEMINAR-Clinical Microbiology: Topic-Human Immuno-Deficiency Virus (HIV)sushant_dharNo ratings yet
- Understanding AIDS and RotavirusDocument34 pagesUnderstanding AIDS and RotavirusCrystal Ann TadiamonNo ratings yet
- Hiv& AidsDocument203 pagesHiv& Aidsclaire wacukaNo ratings yet
- Human Immunodeficiency Virus LectureDocument34 pagesHuman Immunodeficiency Virus Lectureapi-19969058No ratings yet
- Aids and Immunodeficiencies: - Kiruthika ManivannanDocument35 pagesAids and Immunodeficiencies: - Kiruthika ManivannanrevaishNo ratings yet
- Chapter X HivDocument52 pagesChapter X HivD PharmaNo ratings yet
- Understanding Human Retroviruses and HIVDocument58 pagesUnderstanding Human Retroviruses and HIVRandy BerryNo ratings yet
- Antiretroviral Therapy: Awlachew Firde (S.Pharmacist)Document40 pagesAntiretroviral Therapy: Awlachew Firde (S.Pharmacist)wedajoyonas50No ratings yet
- Human Immunodeficiency VirusDocument26 pagesHuman Immunodeficiency ViruspraneethasruthiNo ratings yet
- Session 6 L Blood Borne Viruses HIV HVDocument62 pagesSession 6 L Blood Borne Viruses HIV HVBlendma AhmedNo ratings yet
- Medical Virology Retrovirus HIV/AIDSDocument11 pagesMedical Virology Retrovirus HIV/AIDSAtheer AlabdyNo ratings yet
- Co-Receptor: Cell Surface Receptor LigandDocument11 pagesCo-Receptor: Cell Surface Receptor LigandIS99057No ratings yet
- Manifestasi Klinis HIVDocument111 pagesManifestasi Klinis HIVFebrina EvaNo ratings yet
- Acquired Immunodeficiency SyndromeDocument47 pagesAcquired Immunodeficiency SyndromeEndang SetiawatiNo ratings yet
- MMSU Nursing Students Report on HIV/AIDSDocument10 pagesMMSU Nursing Students Report on HIV/AIDSEyySiEffVee100% (1)
- Adiel Joy P. Calsa (HIV AIDS Output)Document6 pagesAdiel Joy P. Calsa (HIV AIDS Output)Adiel CalsaNo ratings yet
- HIV Engleza BriefDocument108 pagesHIV Engleza BriefOnofrei MariaNo ratings yet
- Overview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieDocument101 pagesOverview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieImanuel Fantevie100% (1)
- Hiv Seminar 2019Document49 pagesHiv Seminar 2019clarice_condeno100% (1)
- Human Immunodeficiency Virus (Hiv)Document50 pagesHuman Immunodeficiency Virus (Hiv)kiran kcNo ratings yet
- Pathophysiology of Hiv and Aids: BY: DR Olasinde Abdulazeez Ayodeji Department of Community Medicine ABUTH ZariaDocument14 pagesPathophysiology of Hiv and Aids: BY: DR Olasinde Abdulazeez Ayodeji Department of Community Medicine ABUTH ZariaSalihu MustaphaNo ratings yet
- Hiv and Aids: ID Specialist Tamar KhuchuaDocument84 pagesHiv and Aids: ID Specialist Tamar KhuchuaMAMA LALANo ratings yet
- Immunology 8Document37 pagesImmunology 8ukashazam19No ratings yet
- Treatment. Neurological ComplicationsDocument39 pagesTreatment. Neurological ComplicationsagueletaNo ratings yet
- DR Anil Sabharwal MDDocument57 pagesDR Anil Sabharwal MDsaump3No ratings yet
- Presented By: Marlene Lombi C T SiviaDocument19 pagesPresented By: Marlene Lombi C T SiviaVanlal RemruatiNo ratings yet
- Serology of HIVDocument59 pagesSerology of HIVDesalegn AshenafiNo ratings yet
- Disease Process HIVDocument4 pagesDisease Process HIValeksdj1987No ratings yet
- N.B. HIV-1 and HIV-2 Are The Two Main Types of HIV. Most People With HIV Have HIV-1. HIV in This Document Refers To HIV-1Document4 pagesN.B. HIV-1 and HIV-2 Are The Two Main Types of HIV. Most People With HIV Have HIV-1. HIV in This Document Refers To HIV-1tenqbroNo ratings yet
- Dengue-Malaria TOT For Doctors 2022 Dengue Diagnosis-Dr - A .NandyDocument32 pagesDengue-Malaria TOT For Doctors 2022 Dengue Diagnosis-Dr - A .NandyAkshat SharmaNo ratings yet
- Biology Ip XiiDocument8 pagesBiology Ip XiiSugumaran MageshNo ratings yet
- HIV AND AIDSDocument23 pagesHIV AND AIDSjigyansh25No ratings yet
- Ate KrissiaDocument15 pagesAte Krissiaroan marie isaacNo ratings yet
- 162 Biology of HIVv2Document3 pages162 Biology of HIVv2gert16No ratings yet
- 05 PiconavirusDocument31 pages05 PiconavirusSAMMYNo ratings yet
- Hiv and Prevention of Mother-To-Child Transmission (PMTCT) : by Gebremaryam TDocument100 pagesHiv and Prevention of Mother-To-Child Transmission (PMTCT) : by Gebremaryam THambal AhamedNo ratings yet
- HIV and AIDS Syndrome - NCBIDocument9 pagesHIV and AIDS Syndrome - NCBIApriani KudiNo ratings yet
- Immune System Human Immunodeficiency Virus: (Acquired Immune Deficiency Syndrome)Document5 pagesImmune System Human Immunodeficiency Virus: (Acquired Immune Deficiency Syndrome)Ampy SuarezNo ratings yet
- Care of Patients Living With HIV - CompressedDocument36 pagesCare of Patients Living With HIV - CompressedJoice DasNo ratings yet
- Human Immunodeficiency VirusDocument64 pagesHuman Immunodeficiency Virusmwambungup100% (2)
- Hiv/Aids and Principles of HaartDocument88 pagesHiv/Aids and Principles of Haarthabtamu alemayehuNo ratings yet
- JUH Residency Exam 2016Document9 pagesJUH Residency Exam 2016Nashaat H. AlshawabkehNo ratings yet
- Generic diabetes medications and trade namesDocument4 pagesGeneric diabetes medications and trade namesMohammadSAL-RawashdehNo ratings yet
- Pathophysiology of Urinary Tract PDFDocument22 pagesPathophysiology of Urinary Tract PDFMohammadSAL-RawashdehNo ratings yet
- Tak&cha&gen&sur&uro&1st PDFDocument321 pagesTak&cha&gen&sur&uro&1st PDFMohammadSAL-RawashdehNo ratings yet
- ملخص عن حب الشبابDocument10 pagesملخص عن حب الشبابMohammadSAL-RawashdehNo ratings yet
- Eau 2020 PDFDocument1,563 pagesEau 2020 PDFMirellaNo ratings yet
- كتاب اسئلة جميلDocument401 pagesكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- 2015 Residancy Exam JUHDocument6 pages2015 Residancy Exam JUHMohammadSAL-RawashdehNo ratings yet
- 2017 Residancy Exam JUHDocument8 pages2017 Residancy Exam JUHMohammadSAL-RawashdehNo ratings yet
- BBM - 978 3 319 23458 8/1 PDFDocument22 pagesBBM - 978 3 319 23458 8/1 PDFmedicalNo ratings yet
- Gillenwater - Adult and Pediatric Urology 4th EdDocument1,564 pagesGillenwater - Adult and Pediatric Urology 4th EdRoxana Boloaga100% (1)
- Chapter #55 - Physiology and Pharmacology of The Renal Pelvis and UreterDocument6 pagesChapter #55 - Physiology and Pharmacology of The Renal Pelvis and UreterMohammadSAL-RawashdehNo ratings yet
- (Mebooksfree - Net) Com&rev&uro&2018 OptimizedDocument851 pages(Mebooksfree - Net) Com&rev&uro&2018 OptimizedMohammadSAL-RawashdehNo ratings yet
- Eur&ass&uro&poc&gui&2020 PDFDocument445 pagesEur&ass&uro&poc&gui&2020 PDFMohammadSAL-RawashdehNo ratings yet
- (Mebooksfree Net) Hin&atl&uro&sur&4thDocument967 pages(Mebooksfree Net) Hin&atl&uro&sur&4thMohammadSAL-Rawashdeh100% (12)
- (Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndDocument1,235 pages(Mebooksfree Net) Pri&pra&uro&sal&2&vol&set&2ndMohammadSAL-Rawashdeh100% (1)
- كتاب اسئلة جميلDocument401 pagesكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- (Mebooksfree Net) Oxf&tex&uro&sur&1stDocument1,201 pages(Mebooksfree Net) Oxf&tex&uro&sur&1stMohammadSAL-Rawashdeh100% (2)
- Urology Sample MCQ Exam eDocument5 pagesUrology Sample MCQ Exam eMohammadSAL-RawashdehNo ratings yet
- Shenimt e Mia Personale Per DDXDocument281 pagesShenimt e Mia Personale Per DDXJeronim H'gharNo ratings yet
- Electrolyte BalanceDocument39 pagesElectrolyte BalanceMohammadSAL-RawashdehNo ratings yet
- Atlas 4 دائرة معارف طبية Reduced PDFDocument316 pagesAtlas 4 دائرة معارف طبية Reduced PDFMohammadSAL-RawashdehNo ratings yet
- Sabers HandbookDocument35 pagesSabers HandbookMohammadSAL-Rawashdeh100% (1)
- أدوية الطوارىءDocument162 pagesأدوية الطوارىءManar22No ratings yet
- 17 - 47 HerniaDocument68 pages17 - 47 HerniaJoseph RichardsonNo ratings yet
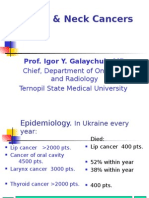
- Head & Neck Cancers: Prof. Igor Y. Galaychuk, MDDocument43 pagesHead & Neck Cancers: Prof. Igor Y. Galaychuk, MDMohammadSAL-RawashdehNo ratings yet
- Shenimt e Mia Personale Per DDXDocument281 pagesShenimt e Mia Personale Per DDXJeronim H'gharNo ratings yet
- 6 - 7 - 8 Peritoneum, Pancreas, AppendixDocument134 pages6 - 7 - 8 Peritoneum, Pancreas, AppendixMohammadSAL-RawashdehNo ratings yet
- Oral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityDocument38 pagesOral Cancer: Oral Cancer Is A Subtype of Head and Neck Cancer, Is Any Cancerous Tissue Growth Located in The Oral CavityMohammadSAL-RawashdehNo ratings yet
- Epidemiology of Cancer. Methods of Diagnosis and TreatmentDocument70 pagesEpidemiology of Cancer. Methods of Diagnosis and TreatmentMohammadSAL-RawashdehNo ratings yet
- Excipients As StabilizersDocument7 pagesExcipients As StabilizersxdgvsdgNo ratings yet
- Evaluation of Personal Dust Exposure of The Rice Mill Workers in AssamDocument10 pagesEvaluation of Personal Dust Exposure of The Rice Mill Workers in AssamIJAMTESNo ratings yet
- Frontier DL650 Maintenance Guide Ver 1.0Document25 pagesFrontier DL650 Maintenance Guide Ver 1.0philippe raynalNo ratings yet
- Narrative Poetry 6305Document14 pagesNarrative Poetry 6305Siti AisyahNo ratings yet
- Read The Following Text. A Day in The Life of Paula Radcliffe - Marathon RunnerDocument2 pagesRead The Following Text. A Day in The Life of Paula Radcliffe - Marathon RunnerAldo JimenezNo ratings yet
- Gas Booster Systems Brochure r7Document12 pagesGas Booster Systems Brochure r7ridwansaungnage_5580No ratings yet
- Refrigeration and Air Conditioning Technology 8th Edition Tomczyk Silberstein Whitman Johnson Solution ManualDocument5 pagesRefrigeration and Air Conditioning Technology 8th Edition Tomczyk Silberstein Whitman Johnson Solution Manualrachel100% (24)
- Drug Study Pre OpDocument6 pagesDrug Study Pre OpgiaNo ratings yet
- 6th Class EM All LessonsDocument33 pages6th Class EM All LessonsSathish PurushothamNo ratings yet
- 310 Ta PDFDocument8 pages310 Ta PDFVincent GomuliaNo ratings yet
- Chapter - 10 NanoshellsDocument13 pagesChapter - 10 NanoshellskarthikNo ratings yet
- Coa Polivinilpirrolidona K-90 (PVP K-90) Lote 20221019Document1 pageCoa Polivinilpirrolidona K-90 (PVP K-90) Lote 20221019Ives AlbarracinNo ratings yet
- UK & India Health Insurance Actuarial ExamDocument4 pagesUK & India Health Insurance Actuarial ExamVignesh SrinivasanNo ratings yet
- KPI and Supplier Performance Scorecard ToolDocument7 pagesKPI and Supplier Performance Scorecard ToolJayant Kumar JhaNo ratings yet
- SureFlo RDocument2 pagesSureFlo RKen NgNo ratings yet
- Cost Estimation of SlaughterhouseDocument25 pagesCost Estimation of Slaughterhousemohamed faahiyeNo ratings yet
- 'S Outfits and Emergency Escape Breathing Devices (Eebd)Document11 pages'S Outfits and Emergency Escape Breathing Devices (Eebd)Thurdsuk NoinijNo ratings yet
- Barangay Peace and Order and Public Safety Plan Bpops Annex ADocument3 pagesBarangay Peace and Order and Public Safety Plan Bpops Annex AImee CorreaNo ratings yet
- PE1 q1 Mod6 ProperEtiquetteand-Safetyinthe-UseofFacilitiesEquip v1-ADMDocument12 pagesPE1 q1 Mod6 ProperEtiquetteand-Safetyinthe-UseofFacilitiesEquip v1-ADMelvira.raagas2No ratings yet
- F 204 (AutoRecovered)Document27 pagesF 204 (AutoRecovered)safiqulislam100% (1)
- Ethics and Disasters: Patricia Reynolds Director, Bishopric Medical Library Sarasota Memorial Hospital Sarasota, FLDocument61 pagesEthics and Disasters: Patricia Reynolds Director, Bishopric Medical Library Sarasota Memorial Hospital Sarasota, FLChandra Prakash JainNo ratings yet
- Case Digest 16Document2 pagesCase Digest 16Mavic MoralesNo ratings yet
- Installation Procedure.Document11 pagesInstallation Procedure.er_paramjeetgillNo ratings yet
- AC7101.1 Rev G 2Document37 pagesAC7101.1 Rev G 2Namelezz ShadowwNo ratings yet
- Carbohidratos - Determinación - Use of The Alditol Acetate Derivatisation For The Analysis of Reducing Sugars in Potato TubersDocument5 pagesCarbohidratos - Determinación - Use of The Alditol Acetate Derivatisation For The Analysis of Reducing Sugars in Potato TubersHernán AstudilloNo ratings yet
- Chapter 3 NotesDocument10 pagesChapter 3 Notesmjamie12345No ratings yet
- Single Inlet Centrifugal FanDocument43 pagesSingle Inlet Centrifugal Fan4uengineerNo ratings yet
- Community Medicine DissertationDocument7 pagesCommunity Medicine DissertationCollegePaperGhostWriterSterlingHeights100% (1)
- Escala de Violencia e Índice de SeveridadDocument11 pagesEscala de Violencia e Índice de SeveridadpsiserviciosprofesioNo ratings yet
- Lit Crit TextDocument8 pagesLit Crit TextFhe CidroNo ratings yet