You might also like
- 07-MAKALAH - Prof DR DR Ismoedijanto SpA (K)Document41 pages07-MAKALAH - Prof DR DR Ismoedijanto SpA (K)Anay TullahNo ratings yet
- POST TERM InfantDocument17 pagesPOST TERM InfantJaya Prabha100% (1)
- Tetanus and Tetanus ToxoidDocument17 pagesTetanus and Tetanus ToxoidhabibiNo ratings yet
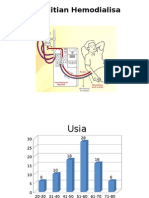
- Penelitian HemodialisaDocument6 pagesPenelitian HemodialisahabibiNo ratings yet
- Hepatitis BDocument47 pagesHepatitis BhabibiNo ratings yet
- MeaslesDocument34 pagesMeasleshabibiNo ratings yet
- Note To Presenters: Images of Vaccine-Preventable Diseases Are Available From The Immunization Action Coalition Website atDocument14 pagesNote To Presenters: Images of Vaccine-Preventable Diseases Are Available From The Immunization Action Coalition Website athabibiNo ratings yet
- Note To Presenters: Images of Vaccine-Preventable Diseases Are Available From The Immunization Action Coalition Website atDocument14 pagesNote To Presenters: Images of Vaccine-Preventable Diseases Are Available From The Immunization Action Coalition Website athabibiNo ratings yet
- 08 Ok-Lap Penlt01-Dr M Ali Faisal PDFDocument2 pages08 Ok-Lap Penlt01-Dr M Ali Faisal PDFAdhitya RevannoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Patient Care Plan: Nursing Diagnosis (In Priority Order) Patient-Centered Goals Nursing Intervention Rationale EvaluationDocument3 pagesPatient Care Plan: Nursing Diagnosis (In Priority Order) Patient-Centered Goals Nursing Intervention Rationale Evaluationmp1757No ratings yet
- Listening ScriptsDocument3 pagesListening ScriptsNghi QuachNo ratings yet
- Aklan Polytechnic College: Performance Rating ScaleDocument3 pagesAklan Polytechnic College: Performance Rating ScaleShane DamianNo ratings yet
- 2019 - 2020 - Boston Immunization - Hult Immunization FormDocument4 pages2019 - 2020 - Boston Immunization - Hult Immunization FormOscar RomainvilleNo ratings yet
- Prosthodontics Q&a (CDD)Document121 pagesProsthodontics Q&a (CDD)Tara Lingating100% (1)
- Philippine Health Insurance CorporationDocument1 pagePhilippine Health Insurance CorporationEJ LomocsoNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument1 pageMaklumat Vaksinasi: Vaccination DetailsZulkarnain KamalNo ratings yet
- 12 The Changing Face of Aesthetic DentistryDocument8 pages12 The Changing Face of Aesthetic DentistryOziel Ramirez OrtegaNo ratings yet
- Handout AtelectasisDocument14 pagesHandout AtelectasisSasha IfahmyNo ratings yet
- Into Sgul Summer Programme Flyer August 2014Document3 pagesInto Sgul Summer Programme Flyer August 2014Maryuri LoteNo ratings yet
- Algoritma CKD PDFDocument2 pagesAlgoritma CKD PDFDesla Citra100% (1)
- Noushad RT-PCR TEST REPORT 2Document2 pagesNoushad RT-PCR TEST REPORT 2kabirNo ratings yet
- Etiology of Mental DisordersDocument10 pagesEtiology of Mental DisordersMuhammad Darussalam DarwisNo ratings yet
- Chapter 29 Prep UDocument6 pagesChapter 29 Prep UPrincess Gwen ZmanNo ratings yet
- Management of Traumatic Dental Injury, Midline Diastema, and Single Tooth Crossbite in A 9 Year Old Child: A Pediatric Dentistry ApproachDocument6 pagesManagement of Traumatic Dental Injury, Midline Diastema, and Single Tooth Crossbite in A 9 Year Old Child: A Pediatric Dentistry ApproachKavanila BilbalqishNo ratings yet
- Organizational Chart Tertiary LabDocument1 pageOrganizational Chart Tertiary LabMiki Nishihara86% (7)
- Notice To Kettle Falls SDDocument2 pagesNotice To Kettle Falls SDErin RobinsonNo ratings yet
- PNLE III For Care of Clients With Physiologic and Psychosocial Alterations (Part 1) 100 ItemaDocument30 pagesPNLE III For Care of Clients With Physiologic and Psychosocial Alterations (Part 1) 100 ItemaIk-ik Miral100% (1)
- Bio DoopDocument6 pagesBio DoopAnaconda Warriors 12 ANo ratings yet
- Resuscitation: Richard A. Field, Zoë Fritz, Annalie Baker, Amy Grove, Gavin D. PerkinsDocument14 pagesResuscitation: Richard A. Field, Zoë Fritz, Annalie Baker, Amy Grove, Gavin D. PerkinsFira GorjessNo ratings yet
- National Physician Fee Schedule Relative Value File Calendar Year 2016Document21 pagesNational Physician Fee Schedule Relative Value File Calendar Year 2016Budi KusumaNo ratings yet
- Cocci VexDocument18 pagesCocci VexNona AlyNo ratings yet
- Nepal Medical College: Affiliated To Kathmandu UniversityDocument3 pagesNepal Medical College: Affiliated To Kathmandu UniversitySachita BudhathokiNo ratings yet
- Health InsuranceDocument40 pagesHealth InsuranceSubhadeep SahaNo ratings yet
- Ballad Scarce Resource Allocation Patient Notification LetterDocument2 pagesBallad Scarce Resource Allocation Patient Notification LetterJosh Smith100% (1)
- Maths IADocument11 pagesMaths IAJúlia de GouvêaNo ratings yet
- Research Study On Knowledge of Interns Regarding Wound CareDocument41 pagesResearch Study On Knowledge of Interns Regarding Wound CareBritten Norman Santiago100% (1)
- Bautista, 2020. Health Literacy Education and Research in The Philippines: An Agenda For Filipino Information Professionals During and After COVID-19Document7 pagesBautista, 2020. Health Literacy Education and Research in The Philippines: An Agenda For Filipino Information Professionals During and After COVID-19kelseyNo ratings yet
- Mast Cell Activation DiseaseDocument8 pagesMast Cell Activation DiseaseJesse FrontierlandNo ratings yet
- 1 4929631937565294920Document986 pages1 4929631937565294920MAURICE022100% (2)