You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Templist Scroll by :dr. Lawiy-Zodok (C) (R) TMDocument144 pagesThe Templist Scroll by :dr. Lawiy-Zodok (C) (R) TM:Lawiy-Zodok:Shamu:-El100% (5)
- (Razavi) Design of Analog Cmos Integrated CircuitsDocument21 pages(Razavi) Design of Analog Cmos Integrated CircuitsNiveditha Nivi100% (1)
- Antonovsky (1979)Document280 pagesAntonovsky (1979)M.Fakhrul Kurnia100% (1)
- Ancient MesopotamiaDocument69 pagesAncient MesopotamiaAlma CayapNo ratings yet
- Elevator Traction Machine CatalogDocument24 pagesElevator Traction Machine CatalogRafif100% (1)
- Draft Initial Study - San Joaquin Apartments and Precinct Improvements ProjectDocument190 pagesDraft Initial Study - San Joaquin Apartments and Precinct Improvements Projectapi-249457935No ratings yet
- Space DynamicsDocument37 pagesSpace Dynamicspurushottam KashyapNo ratings yet
- Qualitative Research EssayDocument9 pagesQualitative Research EssayMichael FoleyNo ratings yet
- Young Women's Sexuality in Perrault and CarterDocument4 pagesYoung Women's Sexuality in Perrault and CarterOuki MilestoneNo ratings yet
- DNB Paper - IDocument7 pagesDNB Paper - Isushil chaudhari100% (7)
- Aacra Draft Preliminary Report PDFDocument385 pagesAacra Draft Preliminary Report PDFBeselam SeyedNo ratings yet
- APLICACIONES PARA AUTOS Y CARGA LIVIANADocument50 pagesAPLICACIONES PARA AUTOS Y CARGA LIVIANApancho50% (2)
- Discuss The Challenges For Firms To Operate in The Hard-Boiled Confectionery Market in India?Document4 pagesDiscuss The Challenges For Firms To Operate in The Hard-Boiled Confectionery Market in India?harryNo ratings yet
- 12 Week Heavy Slow Resistance Progression For Patellar TendinopathyDocument4 pages12 Week Heavy Slow Resistance Progression For Patellar TendinopathyHenrique Luís de CarvalhoNo ratings yet
- 40 26Document3 pages40 26Maxi452No ratings yet
- Flowing Gas Material BalanceDocument4 pagesFlowing Gas Material BalanceVladimir PriescuNo ratings yet
- Phenomenological of in Church and TV WorshipDocument18 pagesPhenomenological of in Church and TV WorshipCindy TirtaNo ratings yet
- 1.2 - Sewing Machine and Special AttachmentsDocument3 pages1.2 - Sewing Machine and Special Attachmentsmaya_muth0% (1)
- Introduction To Finite Element Methods (2001) (En) (489s)Document489 pagesIntroduction To Finite Element Methods (2001) (En) (489s)green77parkNo ratings yet
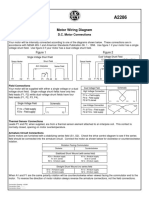
- Motor Wiring Diagram: D.C. Motor ConnectionsDocument1 pageMotor Wiring Diagram: D.C. Motor Connectionsczds6594No ratings yet
- Oral Nutrition Support NotesDocument28 pagesOral Nutrition Support Notesleemon.mary.alipao8695No ratings yet
- Interactive Architecture Adaptive WorldDocument177 pagesInteractive Architecture Adaptive Worldhoma massihaNo ratings yet
- Final Decision W - Cover Letter, 7-14-22Document19 pagesFinal Decision W - Cover Letter, 7-14-22Helen BennettNo ratings yet
- BCP-8000 User's ManualDocument36 pagesBCP-8000 User's ManualAsad PatelNo ratings yet
- Peptic Ulcer Disease: Causes, Symptoms and TreatmentDocument24 pagesPeptic Ulcer Disease: Causes, Symptoms and TreatmentOktaviana Sari Dewi100% (1)
- Features Integration of Differential Binomial: DX BX A X P N MDocument4 pagesFeatures Integration of Differential Binomial: DX BX A X P N Mابو سامرNo ratings yet
- Crew Served WeaponsDocument11 pagesCrew Served WeaponsKyle Fagin100% (1)
- Air Arms S400 EXPDocument3 pagesAir Arms S400 EXPapi-3695814No ratings yet
- Uhf Leaky Feeder Rev CDocument4 pagesUhf Leaky Feeder Rev CLuis Isaac PadillaNo ratings yet