You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- (Problem Books in Mathematics) Antonio Caminha Muniz Neto - An Excursion Through Elementary Mathematics, Volume III - Discrete Mathematics and Polynomial Algebra (2018, Springer)Document647 pages(Problem Books in Mathematics) Antonio Caminha Muniz Neto - An Excursion Through Elementary Mathematics, Volume III - Discrete Mathematics and Polynomial Algebra (2018, Springer)Anonymous iH6noeaX7100% (2)
- MEMORANDUM OF AGREEMENT DraftsDocument3 pagesMEMORANDUM OF AGREEMENT DraftsRichard Colunga80% (5)
- 2010 Information ExchangeDocument15 pages2010 Information ExchangeAnastasia RotareanuNo ratings yet
- TechBridge TCP ServiceNow Business Case - Group 6Document9 pagesTechBridge TCP ServiceNow Business Case - Group 6Takiyah Shealy100% (1)
- What Is The PCB Shelf Life Extending The Life of PCBsDocument9 pagesWhat Is The PCB Shelf Life Extending The Life of PCBsjackNo ratings yet
- E Voting PPT - 1Document11 pagesE Voting PPT - 1madhu100% (2)
- HangersSupportsReferenceDataGuide PDFDocument57 pagesHangersSupportsReferenceDataGuide PDFIndra RosadiNo ratings yet
- CV Ashish PDFDocument3 pagesCV Ashish PDFRoshan KejariwalNo ratings yet
- Docket - CDB Batu GajahDocument1 pageDocket - CDB Batu Gajahfatin rabiatul adawiyahNo ratings yet
- Peanut AllergyDocument4 pagesPeanut AllergyLNICCOLAIONo ratings yet
- Consumer Protection ActDocument34 pagesConsumer Protection ActshikhroxNo ratings yet
- Guidelines For Doing Business in Grenada & OECSDocument14 pagesGuidelines For Doing Business in Grenada & OECSCharcoals Caribbean GrillNo ratings yet
- NCP - Impaired Urinary EliminationDocument3 pagesNCP - Impaired Urinary EliminationFretzgine Lou ManuelNo ratings yet
- Law of AttractionDocument2 pagesLaw of AttractionKate SummersNo ratings yet
- Final - Anarchy One-Sheet Sell SheetDocument2 pagesFinal - Anarchy One-Sheet Sell SheetMaddanie WijayaNo ratings yet
- Agenda - 2 - Presentation - MS - IUT - Thesis Proposal PPT Muhaiminul 171051001Document13 pagesAgenda - 2 - Presentation - MS - IUT - Thesis Proposal PPT Muhaiminul 171051001Tanvir AhmadNo ratings yet
- Ultimate Trading Guide - Flash FUT 2023Document33 pagesUltimate Trading Guide - Flash FUT 2023marciwnw INo ratings yet
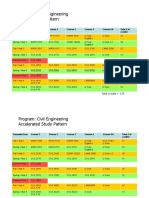
- HKUST 4Y Curriculum Diagram CIVLDocument4 pagesHKUST 4Y Curriculum Diagram CIVLfrevNo ratings yet
- MegaMacho Drums BT READ MEDocument14 pagesMegaMacho Drums BT READ MEMirkoSashaGoggoNo ratings yet
- SHS G11 Reading and Writing Q3 Week 1 2 V1Document15 pagesSHS G11 Reading and Writing Q3 Week 1 2 V1Romeo Espinosa Carmona JrNo ratings yet
- UG ENGLISH Honours PDFDocument59 pagesUG ENGLISH Honours PDFMR.Shantanu SharmaNo ratings yet
- Session 10. Value Proposition.Document69 pagesSession 10. Value Proposition.Bibhu R. TuladharNo ratings yet
- Initial Police Report: Calamba City Police Station Brgy Real, Calamba City, Laguna E-Mail: 545-1694/545-6789 Loc 8071Document1 pageInitial Police Report: Calamba City Police Station Brgy Real, Calamba City, Laguna E-Mail: 545-1694/545-6789 Loc 8071Jurish BunggoNo ratings yet
- 9701 Nos Ps 23Document5 pages9701 Nos Ps 23Hubbak KhanNo ratings yet
- Legrand Price List-01 ST April-2014Document144 pagesLegrand Price List-01 ST April-2014Umesh SutharNo ratings yet
- Wordbank 15 Coffee1Document2 pagesWordbank 15 Coffee1akbal13No ratings yet
- Visi RuleDocument6 pagesVisi RuleBruce HerreraNo ratings yet
- ES Parent Bulletin Vol#19 2012 May 25Document13 pagesES Parent Bulletin Vol#19 2012 May 25International School ManilaNo ratings yet
- Role of Communication at Mahabharatha WarDocument19 pagesRole of Communication at Mahabharatha WarAmit Kalita50% (2)
- Vest3000mkii TurntableDocument16 pagesVest3000mkii TurntableElkin BabiloniaNo ratings yet