You might also like
- Fistula Definition, Causes, Types and TreatmentDocument27 pagesFistula Definition, Causes, Types and TreatmentRaissa Pauline Oliva0% (1)
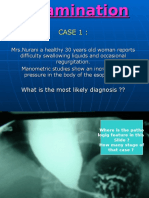
- Difficulty swallowing and regurgitationDocument36 pagesDifficulty swallowing and regurgitationrossy3lamerkabelNo ratings yet
- Crohn's Disease: Cobblestoning (Ulceronodular Pattern)Document5 pagesCrohn's Disease: Cobblestoning (Ulceronodular Pattern)rossy3lamerkabelNo ratings yet
- Crohn's Disease: Cobblestoning (Ulceronodular Pattern)Document5 pagesCrohn's Disease: Cobblestoning (Ulceronodular Pattern)rossy3lamerkabelNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Teaching Project - BPDocument22 pagesTeaching Project - BPapi-283482759No ratings yet
- Schizophrenia - Practice Essentials, Background, PathophysiologyDocument10 pagesSchizophrenia - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Fungal Keratitis in FarmerDocument4 pagesFungal Keratitis in FarmerChikita Rizqi HanifatiNo ratings yet
- Neonatal JaundiceDocument22 pagesNeonatal JaundiceNivedita Charan100% (1)
- E-Poster PresentationDocument1 pageE-Poster PresentationOvamelia JulioNo ratings yet
- Embryology MCQDocument10 pagesEmbryology MCQTofik MohammedNo ratings yet
- Pharmaceutical Assasination (Partial)Document14 pagesPharmaceutical Assasination (Partial)jamie_clark_2100% (2)
- MESOTHERAPYDocument39 pagesMESOTHERAPYAtid Amanda100% (2)
- OECD 404 Acute Dermal Irritation TestDocument5 pagesOECD 404 Acute Dermal Irritation TestTejas ShirsathNo ratings yet
- NDT 3 429Document13 pagesNDT 3 429Mohammed AldaffaieNo ratings yet
- Managing Pain After AppendectomyDocument2 pagesManaging Pain After AppendectomyChatoh SanaoNo ratings yet
- Pediatric Cardiac Patients: History TakingDocument31 pagesPediatric Cardiac Patients: History TakingnovylatifahNo ratings yet
- 1 Hygene and SanitationDocument22 pages1 Hygene and SanitationJammil Ud-ulonNo ratings yet
- Activity No. 7.1 BloodDocument2 pagesActivity No. 7.1 BloodDree SermanNo ratings yet
- MODUL 1 FKG UnairDocument61 pagesMODUL 1 FKG UnairLaurensia NovenNo ratings yet
- Njala University: Bo Campus-Kowama LocationDocument32 pagesNjala University: Bo Campus-Kowama LocationALLIEU FB SACCOHNo ratings yet
- New Microsoft Office Word DocumentDocument2 pagesNew Microsoft Office Word DocumentAnam BukhariNo ratings yet
- Maritime Declaration of HealthDocument1 pageMaritime Declaration of HealthKarym DangerousNo ratings yet
- NLR As Biomarker of DeleriumDocument9 pagesNLR As Biomarker of DeleriumbrendaNo ratings yet
- Head Eyes: Head To Toe AssessmentDocument2 pagesHead Eyes: Head To Toe AssessmentVijungco88% (8)
- Halozyme Therapeutics, Inc. 2009 Investor Day PresentationDocument88 pagesHalozyme Therapeutics, Inc. 2009 Investor Day Presentationsstrumello7395No ratings yet
- Abbas Et Al. 2020 - Nature Immunology-2020-Abbas-TomaselloDocument33 pagesAbbas Et Al. 2020 - Nature Immunology-2020-Abbas-TomaselloAchille BroggiNo ratings yet
- Nitsbin(ንጽቢን) I. Medicine 1st Edition - (Revised)-1Document1,380 pagesNitsbin(ንጽቢን) I. Medicine 1st Edition - (Revised)-1bedanetibeso0No ratings yet
- Microbiology Quick TableDocument2 pagesMicrobiology Quick TableCoy Nuñez100% (2)
- Drug Study Quinine SulfateDocument7 pagesDrug Study Quinine SulfateKathlyn_Matic_6376No ratings yet
- GBS A ReviewDocument6 pagesGBS A ReviewNurul Kartika SariNo ratings yet
- Porose Gravidez e Puerperio 2021Document15 pagesPorose Gravidez e Puerperio 2021Ben-Hur AlbergariaNo ratings yet
- Med Surg Test AnswersDocument9 pagesMed Surg Test AnswersAshley Rose100% (3)
- Lip LesionsDocument4 pagesLip LesionsGhada AlqrnawiNo ratings yet
- Triada de CharcotDocument1 pageTriada de Charcotdanitza pilcoNo ratings yet