You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Anatomy & Physiology - Helen McGuinness - Hodder Education (2018)Document370 pagesAnatomy & Physiology - Helen McGuinness - Hodder Education (2018)Teresa Chao100% (4)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Anatomy and PhysiologyDocument8 pagesAnatomy and PhysiologyNeil Ceniza Saile100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pearl CultureDocument85 pagesPearl Culturemorisrav23No ratings yet
- Galeazzi Fracture and Monteggia FractureDocument31 pagesGaleazzi Fracture and Monteggia FracturenihthaNo ratings yet
- Inferior Alveolar Nerve BlockDocument7 pagesInferior Alveolar Nerve BlockSyedMuhammadJunaidNo ratings yet
- 7.0 Tesla MRI Brain AtlasDocument569 pages7.0 Tesla MRI Brain AtlasJosé Luis Chaves100% (4)
- Limb Length DiscrepancyDocument8 pagesLimb Length DiscrepancyManish Prasad100% (1)
- Traction: Dr.K.Arvind Natarajan 1 Year MS OrthoDocument30 pagesTraction: Dr.K.Arvind Natarajan 1 Year MS OrthoKarthick50% (2)
- Cotton OsteotomyDocument16 pagesCotton OsteotomybaoNo ratings yet
- DKBM IndonesiaDocument25 pagesDKBM IndonesiaBagas Andriyono100% (1)
- DKBM IndonesiaDocument25 pagesDKBM IndonesiaBagas Andriyono100% (1)
- Case ReportDocument28 pagesCase Reportgraceswan100% (1)
- 8.anterior GuidanceDocument15 pages8.anterior GuidanceVikas AggarwalNo ratings yet
- MastectomyDocument6 pagesMastectomyJustinAlmedaNo ratings yet
- Pathology and Genetics of Head and Neck TumoursDocument435 pagesPathology and Genetics of Head and Neck TumoursMonica MehendirattaNo ratings yet
- Diskusi Topik Dr. KholisDocument29 pagesDiskusi Topik Dr. KholisgraceswanNo ratings yet
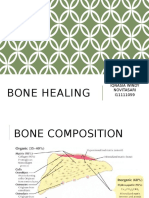
- Bone HealingDocument31 pagesBone HealinggraceswanNo ratings yet
- Journal Reading - AnemiaDocument31 pagesJournal Reading - AnemiagraceswanNo ratings yet
- Tumor Kepala Dan LeherDocument22 pagesTumor Kepala Dan LehergraceswanNo ratings yet
- Open FractureDocument20 pagesOpen FracturegraceswanNo ratings yet
- Abdominal Cutaneous Nerve Entrapment Syndrome (ACNES) : A Commonly Overlooked Cause of Abdominal PainDocument8 pagesAbdominal Cutaneous Nerve Entrapment Syndrome (ACNES) : A Commonly Overlooked Cause of Abdominal PaingraceswanNo ratings yet
- Tumor ParuDocument20 pagesTumor ParugraceswanNo ratings yet
- 203 382 1 SMDocument9 pages203 382 1 SMNajwan Ihsan YPasNo ratings yet
- Chpt08 Id Characterization StreppneumoDocument14 pagesChpt08 Id Characterization StreppneumograceswanNo ratings yet
- Seajphv 2 N 2Document60 pagesSeajphv 2 N 2graceswanNo ratings yet
- Typhoid FeverDocument13 pagesTyphoid FevergraceswanNo ratings yet
- Emergence of Resistant Shigella Dysentriae Bacteria in The IDP CampsDocument2 pagesEmergence of Resistant Shigella Dysentriae Bacteria in The IDP CampsgraceswanNo ratings yet
- Six Newly Recognized Types of Streptococcus PneumoniaeDocument4 pagesSix Newly Recognized Types of Streptococcus PneumoniaegraceswanNo ratings yet
- Pharmacologic Treatment of Chorea in Huntington'S Disease: Drug WarningsDocument2 pagesPharmacologic Treatment of Chorea in Huntington'S Disease: Drug WarningsgraceswanNo ratings yet
- Streptococcous General MethodsDocument69 pagesStreptococcous General MethodsPraveen KumarNo ratings yet
- Penyakit Inf Saluran Pencernaan PDFDocument9 pagesPenyakit Inf Saluran Pencernaan PDFAde PermanaNo ratings yet
- UnicefDocument61 pagesUnicefUgaugaaNo ratings yet
- Child Poverty and DisparitiesDocument300 pagesChild Poverty and DisparitiesgraceswanNo ratings yet
- 1712Document2 pages1712graceswanNo ratings yet
- Okehasbarinda Hasan 08 24Document24 pagesOkehasbarinda Hasan 08 24graceswanNo ratings yet
- Kuliah & Praktikum Modul Gastrointestinal: Windy Novita I11111059Document1 pageKuliah & Praktikum Modul Gastrointestinal: Windy Novita I11111059graceswanNo ratings yet
- 1712Document2 pages1712graceswanNo ratings yet
- JurnalDocument8 pagesJurnalRandy Nugraha Pratama100% (1)
- JurnalDocument8 pagesJurnalRandy Nugraha Pratama100% (1)
- JurnalDocument13 pagesJurnalHaerul Amri HukmanNo ratings yet
- 1983 Speth (Garnsey Bison Kill BOOK)Document255 pages1983 Speth (Garnsey Bison Kill BOOK)jdspethNo ratings yet
- Achilles SpeedBridge™Document6 pagesAchilles SpeedBridge™Nicușor AnghelNo ratings yet
- AAMMJTennis Elbow Everywhere Nov05 P 127-130Document4 pagesAAMMJTennis Elbow Everywhere Nov05 P 127-130Dr A Breck McKayNo ratings yet
- 253 A New Species of Euscorpius Thorell, 1876 (Scorpiones, Euscorpiidae) From ItalyDocument7 pages253 A New Species of Euscorpius Thorell, 1876 (Scorpiones, Euscorpiidae) From ItalyPizza, Mandolino, Berlusconi MussoliniNo ratings yet
- Double-Skin Paddle RadialDocument8 pagesDouble-Skin Paddle RadialSadia GullNo ratings yet
- Vietnamese Species of The Genus AcanthomDocument11 pagesVietnamese Species of The Genus Acanthomminh quang đặngNo ratings yet
- Anthropometric, Strength, Endurance and Flexibility Characteristics of Elite and Recreational ClimbersDocument9 pagesAnthropometric, Strength, Endurance and Flexibility Characteristics of Elite and Recreational Climberschirusa14No ratings yet
- AOSpine Thoracolumbar Classification System - Poster PDFDocument1 pageAOSpine Thoracolumbar Classification System - Poster PDFmhmiguelNo ratings yet
- Anterolateral Approach of Proximal Humerus + Henry ApproachDocument33 pagesAnterolateral Approach of Proximal Humerus + Henry ApproachwildanmalikNo ratings yet
- PE2 Course-PackDocument49 pagesPE2 Course-PackJohn Ian Nisnisan100% (1)
- Biology of Coccinellidae PDFDocument309 pagesBiology of Coccinellidae PDFelena100% (1)
- Symmetry in BiologyDocument5 pagesSymmetry in Biologytr4lNo ratings yet
- Chapter 1 AnatomyDocument83 pagesChapter 1 Anatomymedic99No ratings yet
- Ace PDFDocument684 pagesAce PDFsami xNo ratings yet
- 'Reading' Cross-Sections: Background of The ViewersDocument2 pages'Reading' Cross-Sections: Background of The ViewersPriyanshu SinghNo ratings yet
- Part - I Biology and Culture of Abalone Species and Their Geographical DistributionDocument82 pagesPart - I Biology and Culture of Abalone Species and Their Geographical DistributionLaila UbandoNo ratings yet
- Complete Dentures: Arthur RussellDocument11 pagesComplete Dentures: Arthur RussellGermán PuigNo ratings yet
- CT ProtocolsDocument37 pagesCT ProtocolsSehar GulNo ratings yet
- PP Vs Quinones 183SCRA747Document5 pagesPP Vs Quinones 183SCRA747robdeqNo ratings yet