You might also like
- The Templist Scroll by :dr. Lawiy-Zodok (C) (R) TMDocument144 pagesThe Templist Scroll by :dr. Lawiy-Zodok (C) (R) TM:Lawiy-Zodok:Shamu:-El100% (5)
- Panasonic 2012 PDP Troubleshooting Guide ST50 ST Series (TM)Document39 pagesPanasonic 2012 PDP Troubleshooting Guide ST50 ST Series (TM)Gordon Elder100% (5)
- HSC 405 Grant ProposalDocument23 pagesHSC 405 Grant Proposalapi-355220460100% (2)
- Aircraft Design Project 2Document80 pagesAircraft Design Project 2Technology Informer90% (21)
- 1.2 - Sewing Machine and Special AttachmentsDocument3 pages1.2 - Sewing Machine and Special Attachmentsmaya_muth0% (1)
- Spleen PowerpointDocument30 pagesSpleen PowerpointZakira Alberto100% (1)
- Blood TransfusionDocument58 pagesBlood Transfusionmsat72100% (12)
- Theoretical and Actual CombustionDocument14 pagesTheoretical and Actual CombustionErma Sulistyo R100% (1)
- Elevator Traction Machine CatalogDocument24 pagesElevator Traction Machine CatalogRafif100% (1)
- 11 Baby Crochet Cocoon Patterns PDFDocument39 pages11 Baby Crochet Cocoon Patterns PDFIoanaNo ratings yet
- Schwartz Chapter 33 SpleenDocument20 pagesSchwartz Chapter 33 SpleenGay Solas Epalan100% (1)
- Anemia HemolitikDocument83 pagesAnemia HemolitikWinda A. PanjaitanNo ratings yet
- Antonovsky (1979)Document280 pagesAntonovsky (1979)M.Fakhrul Kurnia100% (1)
- Gautam Samhita CHP 1 CHP 2 CHP 3 ColorDocument22 pagesGautam Samhita CHP 1 CHP 2 CHP 3 ColorSaptarishisAstrology100% (1)
- ThrombophiliaDocument46 pagesThrombophiliaNabelle MarieNo ratings yet
- 9a. Red Cell DisordersDocument46 pages9a. Red Cell DisordersMuhammad DaviqNo ratings yet
- Red Cell Disorders GuideDocument49 pagesRed Cell Disorders GuideGeraldine AgpesNo ratings yet
- Null 1Document49 pagesNull 1ImamAbdyNo ratings yet
- Blood ProductsDocument70 pagesBlood Productsjadhamade339No ratings yet
- Aplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreDocument26 pagesAplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreSandeep m rNo ratings yet
- Aplastic Anemia Lecture 1aDocument39 pagesAplastic Anemia Lecture 1aniaaseta100% (2)
- An Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutDocument77 pagesAn Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutYen-Jen SungNo ratings yet
- Approach To Anemia: Bisrat DDocument45 pagesApproach To Anemia: Bisrat Dyared getachewNo ratings yet
- Thalassemia IAPDocument25 pagesThalassemia IAPAbhishek Gohel100% (1)
- Approuch Anemia PBLDocument31 pagesApprouch Anemia PBLAndy XiaoNo ratings yet
- Hemolytic AnemiaDocument61 pagesHemolytic AnemiaMangayarkarasi ChandrakasanNo ratings yet
- Anaesthetic Implications in Concurrent DiseasesDocument37 pagesAnaesthetic Implications in Concurrent DiseasesJeevan KumarNo ratings yet
- ICU Blood Transfusion & Electrolytes DisturbanceDocument26 pagesICU Blood Transfusion & Electrolytes Disturbancef6080683No ratings yet
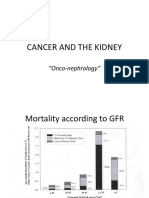
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]No ratings yet
- Pancytopenia: Edwin S. Trinidad, M.D., FPCP, DPSHBTDocument39 pagesPancytopenia: Edwin S. Trinidad, M.D., FPCP, DPSHBTfachrie saputraNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaAshish SoniNo ratings yet
- Handout 2 1522436248 PDFDocument82 pagesHandout 2 1522436248 PDFHarnadi WonogiriNo ratings yet
- Chronic Leukemia: Dr. SamirDocument27 pagesChronic Leukemia: Dr. Samirविजय मैनालीNo ratings yet
- Topic 2. CBC Part 1 2021-02-26 at 11.03.32 PMDocument113 pagesTopic 2. CBC Part 1 2021-02-26 at 11.03.32 PMSub 7 Grp 3No ratings yet
- Topic 6 - Anemia 1Document24 pagesTopic 6 - Anemia 1Vince Martin ManaigNo ratings yet
- Haematological Malignancies: Classification, Clinical Features and ManagementDocument54 pagesHaematological Malignancies: Classification, Clinical Features and ManagementSaifSeddikiNo ratings yet
- Lecture 5.1 Hemolytic Anemia MMDocument41 pagesLecture 5.1 Hemolytic Anemia MMMoeed AliNo ratings yet
- Diagnosing Pancytopenia and Aplastic AnemiaDocument20 pagesDiagnosing Pancytopenia and Aplastic Anemiaroihan iqbalNo ratings yet
- Gangguan TrombositDocument47 pagesGangguan TrombositLayli Nur ArniatiNo ratings yet
- Blood TransfusionDocument57 pagesBlood Transfusionibzshan_No ratings yet
- Acute Myeloid LuekemiaDocument30 pagesAcute Myeloid LuekemiaKathleen DimacaliNo ratings yet
- Bone Marrow Failure 2008-09Document15 pagesBone Marrow Failure 2008-09Karan BhattNo ratings yet
- Blood Transfusion Complications & Management (40Document30 pagesBlood Transfusion Complications & Management (40kushalNo ratings yet
- Ha I by AbdifatahDocument109 pagesHa I by AbdifatahAbdifatah AhmedNo ratings yet
- Curs 6 PDFDocument62 pagesCurs 6 PDFIoanaVioletaDraguNo ratings yet
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- Congenital Hemolytic Anemia GuideDocument37 pagesCongenital Hemolytic Anemia GuideSomendra Mohan ShuklaNo ratings yet
- Anemia Hemolytic - Dr. MulatDocument83 pagesAnemia Hemolytic - Dr. MulatbolabundarNo ratings yet
- Clinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaDocument24 pagesClinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaAhmed. Masud.OthmanNo ratings yet
- Peripheral Smear Review: Diagnostic Aid for Blood DisordersTITLEDocument31 pagesPeripheral Smear Review: Diagnostic Aid for Blood DisordersTITLEDaniel McFarlandNo ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Schwartz's Principles of Surgery 11th Ed. The SpleenDocument54 pagesSchwartz's Principles of Surgery 11th Ed. The SpleenMuhammad Fhandeka IsrarNo ratings yet
- HEMATOPATHOLOGYDocument33 pagesHEMATOPATHOLOGYkiflomNo ratings yet
- Blood Components - DR. ETU-EFEOTOR T. P.Document40 pagesBlood Components - DR. ETU-EFEOTOR T. P.Princewill Seiyefa100% (1)
- PCV and Myeloproliferative IllnessDocument34 pagesPCV and Myeloproliferative Illnessswathi bsNo ratings yet
- HEMADocument44 pagesHEMAJilycamae COSMODNo ratings yet
- In Practice Blood Transfusion in Dogs and Cats1Document7 pagesIn Practice Blood Transfusion in Dogs and Cats1何元No ratings yet
- 6.blood Transfusion, Hemostasis & Coagulation DisordersDocument42 pages6.blood Transfusion, Hemostasis & Coagulation DisordersEyouel TadesseNo ratings yet
- Blood Transfusion Reaction 3032018Document33 pagesBlood Transfusion Reaction 3032018Kelly YeowNo ratings yet
- Multiple Mieloma Dan PVDocument20 pagesMultiple Mieloma Dan PVariienndrrahanniieNo ratings yet
- Aplastic Anemia: Causes, Symptoms and TreatmentDocument16 pagesAplastic Anemia: Causes, Symptoms and TreatmentSetsuna F SeieiNo ratings yet
- Article of Macrocytosis NewDocument9 pagesArticle of Macrocytosis NewMominah MayamNo ratings yet
- The Spleen: Schwartz's Principles of Surgery 11th EdDocument54 pagesThe Spleen: Schwartz's Principles of Surgery 11th EdaddelinsNo ratings yet
- Anemia in SurgeryDocument29 pagesAnemia in SurgeryEdwin OkonNo ratings yet
- Guide to Transfusions and CoagulopathiesDocument10 pagesGuide to Transfusions and Coagulopathieskep1313No ratings yet
- Background of The Study Statement of ObjectivesDocument4 pagesBackground of The Study Statement of ObjectivesEudelyn MelchorNo ratings yet
- GLOBAL Hydro Turbine Folder enDocument4 pagesGLOBAL Hydro Turbine Folder enGogyNo ratings yet
- 1010 PDS WLBP 170601-EN PDFDocument4 pages1010 PDS WLBP 170601-EN PDFIan WoodsNo ratings yet
- Brochure Personal CareDocument38 pagesBrochure Personal CarechayanunNo ratings yet
- Introduction To Finite Element Methods (2001) (En) (489s)Document489 pagesIntroduction To Finite Element Methods (2001) (En) (489s)green77parkNo ratings yet
- 07.03.09 Chest Physiotherapy PDFDocument9 pages07.03.09 Chest Physiotherapy PDFRakesh KumarNo ratings yet
- Oral Nutrition Support NotesDocument28 pagesOral Nutrition Support Notesleemon.mary.alipao8695No ratings yet
- Final Decision W - Cover Letter, 7-14-22Document19 pagesFinal Decision W - Cover Letter, 7-14-22Helen BennettNo ratings yet
- Sri Radhakrishna SwamijiDocument43 pagesSri Radhakrishna SwamijiNarayana IyengarNo ratings yet
- The Impact of Employees' Commitment Towards Food Safety at Ayana Resort, BaliDocument58 pagesThe Impact of Employees' Commitment Towards Food Safety at Ayana Resort, Balirachelle agathaNo ratings yet
- Gas Natural Aplicacion Industria y OtrosDocument319 pagesGas Natural Aplicacion Industria y OtrosLuis Eduardo LuceroNo ratings yet
- Lec9-Rock Cutting ToolsDocument35 pagesLec9-Rock Cutting ToolsAmraha NoorNo ratings yet
- Ro-Buh-Qpl: Express WorldwideDocument3 pagesRo-Buh-Qpl: Express WorldwideverschelderNo ratings yet
- Magnetic Pick UpsDocument4 pagesMagnetic Pick UpslunikmirNo ratings yet
- Sattvik Brochure - Web VersionDocument4 pagesSattvik Brochure - Web Versionudiptya_papai2007No ratings yet
- Phenomenological of in Church and TV WorshipDocument18 pagesPhenomenological of in Church and TV WorshipCindy TirtaNo ratings yet
- Embankment PDFDocument5 pagesEmbankment PDFTin Win HtutNo ratings yet
- The Art of Now: Six Steps To Living in The MomentDocument5 pagesThe Art of Now: Six Steps To Living in The MomentGiovanni AlloccaNo ratings yet
- STS Chapter 1 ReviewerDocument4 pagesSTS Chapter 1 ReviewerEunice AdagioNo ratings yet
- Library Dissertation in Community DentistryDocument9 pagesLibrary Dissertation in Community DentistryPayForPaperCanada100% (1)