You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Wound ManagementDocument3 pagesWound ManagementAmina ThayyibaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 2.early Pregnancy Bleeding and AbortionDocument34 pages2.early Pregnancy Bleeding and AbortionSalman MajidNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Behaviour TherapyDocument32 pagesBehaviour TherapySalman MajidNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Diabetes KetoacidosisDocument23 pagesDiabetes KetoacidosisSalman MajidNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Issue 1 - Amsun Gazette - Editorial TeamDocument14 pagesIssue 1 - Amsun Gazette - Editorial TeamSalman MajidNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Liquid BiopsyDocument2 pagesLiquid BiopsySalman MajidNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Kenya-Comprehensive Multi-Year Plan For 2011-2015 - Year UnknownDocument76 pagesKenya-Comprehensive Multi-Year Plan For 2011-2015 - Year UnknownSalman MajidNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Group 2 Topic 2 3d Group PresentationDocument23 pagesGroup 2 Topic 2 3d Group PresentationSalman MajidNo ratings yet
- Rumenotomy Report SampleDocument5 pagesRumenotomy Report SampleSalman MajidNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Cns PathologyDocument1 pageCns PathologySalman MajidNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Final Report-Brian KenyaDocument78 pagesFinal Report-Brian KenyaSalman MajidNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Pathology of Blood and Lymphatic VesselsDocument55 pagesPathology of Blood and Lymphatic VesselsMhinory OctNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Adult Brain Tumours: DR M.P. Okemwa PathologistDocument39 pagesAdult Brain Tumours: DR M.P. Okemwa PathologistSalman MajidNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Cellular Reaction To InjuryDocument34 pagesCellular Reaction To InjurySalman MajidNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Cholera and Bacillary DysenteryDocument38 pagesCholera and Bacillary DysenterySalman MajidNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Mod3NutriAssess June2010 FinalDocument51 pagesMod3NutriAssess June2010 FinalSalman MajidNo ratings yet
- Introduction To Principles of PathologyDocument16 pagesIntroduction To Principles of PathologySalman MajidNo ratings yet
- A Approach To A Patient - AnaemiaDocument22 pagesA Approach To A Patient - AnaemiaSalman MajidNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Congenital Heart DiseaseDocument43 pagesCongenital Heart DiseaseSalman Majid100% (1)
- Oncogenic VirusesDocument37 pagesOncogenic VirusesSalman Majid0% (1)
- Motor Vehicle Accident PaperworkDocument2 pagesMotor Vehicle Accident PaperworkSalman MajidNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Cardio Exam Checklist2 PDFDocument1 pageCardio Exam Checklist2 PDFDawoodAslamNo ratings yet
- Viral HepatitisDocument57 pagesViral HepatitisSalman MajidNo ratings yet
- PrionsDocument20 pagesPrionsSalman MajidNo ratings yet
- 1B. Culture MethodsDocument18 pages1B. Culture MethodsSalman MajidNo ratings yet
- 1-Intro To Forensic SciDocument46 pages1-Intro To Forensic SciSalman MajidNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- CitrobacterDocument7 pagesCitrobacterSalman MajidNo ratings yet
- Haemoglobin Structure and FunctionDocument7 pagesHaemoglobin Structure and FunctionSalman MajidNo ratings yet
- CephaloVanco PrinceDocument8 pagesCephaloVanco PrinceSalman MajidNo ratings yet
- Process Strategy: Powerpoint Slides by Jeff HeylDocument13 pagesProcess Strategy: Powerpoint Slides by Jeff HeylMuizzNo ratings yet
- DxDiag Copy MSIDocument45 pagesDxDiag Copy MSITạ Anh TuấnNo ratings yet
- How Can Literary Spaces Support Neurodivergent Readers and WritersDocument2 pagesHow Can Literary Spaces Support Neurodivergent Readers and WritersRenato Jr Bernadas Nasilo-anNo ratings yet
- Will Smith BiographyDocument11 pagesWill Smith Biographyjhonatan100% (1)
- REAL BABY FOOD: Easy All-Natural Recipes For Your Baby and Toddler by Jenna HelwigDocument8 pagesREAL BABY FOOD: Easy All-Natural Recipes For Your Baby and Toddler by Jenna HelwigHoughton Mifflin Harcourt Cookbooks50% (2)
- Invoices For UEG IstanbulDocument7 pagesInvoices For UEG IstanbulIesaw IesawNo ratings yet
- Accounting Worksheet Problem 4Document19 pagesAccounting Worksheet Problem 4RELLON, James, M.100% (1)
- Jurnal Ekologi TerestrialDocument6 pagesJurnal Ekologi TerestrialFARIS VERLIANSYAHNo ratings yet
- Protection in Distributed GenerationDocument24 pagesProtection in Distributed Generationbal krishna dubeyNo ratings yet
- Addition Color by Code: Yellow 1, 2, Blue 3, 4, Pink 5, 6 Peach 7, 8 Light Green 9, 10, Black 11Document1 pageAddition Color by Code: Yellow 1, 2, Blue 3, 4, Pink 5, 6 Peach 7, 8 Light Green 9, 10, Black 11Noor NadhirahNo ratings yet
- Homework 1Document8 pagesHomework 1Yooncheul JeungNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Docsity Detailed Lesson Plan 5Document4 pagesDocsity Detailed Lesson Plan 5Sydie MoredoNo ratings yet
- Report On Marketing Strategy of Nestle MILKPAKDocument13 pagesReport On Marketing Strategy of Nestle MILKPAKAzeem Ahmad100% (1)
- Migne. Patrologiae Cursus Completus: Series Latina. 1800. Volume 51.Document516 pagesMigne. Patrologiae Cursus Completus: Series Latina. 1800. Volume 51.Patrologia Latina, Graeca et OrientalisNo ratings yet
- OVDT Vs CRT - GeneralDocument24 pagesOVDT Vs CRT - Generaljaiqc100% (1)
- Terminal Blocks: Assembled Terminal Block and SeriesDocument2 pagesTerminal Blocks: Assembled Terminal Block and SeriesQuan Nguyen TheNo ratings yet
- BIOBASE Vortex Mixer MX-S - MX-F User ManualDocument10 pagesBIOBASE Vortex Mixer MX-S - MX-F User Manualsoporte03No ratings yet
- The Grass Rink Summer Final 2019Document9 pagesThe Grass Rink Summer Final 2019api-241553699No ratings yet
- Electric Vehicles PresentationDocument10 pagesElectric Vehicles PresentationVIBHU CHANDRANSH BHANOT100% (1)
- Taylor Et Al v. Acxiom Corporation Et Al - Document No. 91Document40 pagesTaylor Et Al v. Acxiom Corporation Et Al - Document No. 91Justia.comNo ratings yet
- CEN and CENELEC Position Paper On The Proposal For CPR RevisionDocument15 pagesCEN and CENELEC Position Paper On The Proposal For CPR Revisionhalexing5957No ratings yet
- 1996 OKI LCD Driver Controller DatabookDocument232 pages1996 OKI LCD Driver Controller Databookpiptendo100% (1)
- Rare Malignant Glomus Tumor of The Esophagus With PulmonaryDocument6 pagesRare Malignant Glomus Tumor of The Esophagus With PulmonaryRobrigo RexNo ratings yet
- How To Present A Paper at An Academic Conference: Steve WallaceDocument122 pagesHow To Present A Paper at An Academic Conference: Steve WallaceJessicaAF2009gmtNo ratings yet
- Dialog InggrisDocument4 pagesDialog Inggrisبايو سيتياوانNo ratings yet
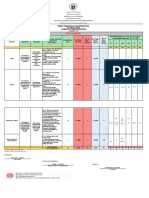
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Document6 pagesRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoNo ratings yet
- Daikin FUW Cabinet Fan Coil UnitDocument29 pagesDaikin FUW Cabinet Fan Coil UnitPaul Mendoza100% (1)
- Toxemias of PregnancyDocument3 pagesToxemias of PregnancyJennelyn LumbreNo ratings yet
- Industrial Machine and ControlsDocument31 pagesIndustrial Machine and ControlsCarol Soi100% (4)