You might also like
- Solutions For All Life Sciences Grade 11 Learners BookDocument73 pagesSolutions For All Life Sciences Grade 11 Learners BookJustinCase19910% (2)
- 2.6.7. Mycoplasmas PDFDocument4 pages2.6.7. Mycoplasmas PDFamerican_guy10No ratings yet
- Vaccines - From Concept To Clinic - L. Paoletti, P. McInnes (CRC, 1999) WW PDFDocument210 pagesVaccines - From Concept To Clinic - L. Paoletti, P. McInnes (CRC, 1999) WW PDFPatriciaNo ratings yet
- Ewing's Sarcoma: A Rare Bone CancerDocument16 pagesEwing's Sarcoma: A Rare Bone CancerChacha Zakiya100% (1)
- Laryngitis Awareness and TreatmentDocument40 pagesLaryngitis Awareness and TreatmentMikhail Guidicelli100% (1)
- Immuno Virology BacteriologyDocument309 pagesImmuno Virology BacteriologyJulianna MacintyreNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- TuberculosisDocument28 pagesTuberculosisbuddysmbdNo ratings yet
- Typhoid Fever Case Study in a ChildDocument43 pagesTyphoid Fever Case Study in a ChildJef Sembrano DiplomaNo ratings yet
- Measles (Rubeola) VirusDocument16 pagesMeasles (Rubeola) Virusstudymedic100% (1)
- Hiv Case StudyDocument2 pagesHiv Case Studyapi-485814878No ratings yet
- Lower Respiratory InfectionsDocument44 pagesLower Respiratory Infectionstummalapalli venkateswara raoNo ratings yet
- A Case Study On DengueDocument11 pagesA Case Study On DengueYetTamparong100% (1)
- Chickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella ZosterDocument12 pagesChickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella Zostersubbu2raj3372100% (2)
- Typhoid FeverDocument68 pagesTyphoid FeverLd Rachel PableoNo ratings yet
- Dengue Hemorrhagic FeverDocument12 pagesDengue Hemorrhagic FeverJohn Maurice AbelNo ratings yet
- Cavite State University: I. ObjectivesDocument7 pagesCavite State University: I. ObjectivesChamy CruzNo ratings yet
- Management of patients with meningitis and encephalitisDocument71 pagesManagement of patients with meningitis and encephalitisSachin DwivediNo ratings yet
- Amoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Document25 pagesAmoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Abdullah AzeemNo ratings yet
- AsthmaDocument20 pagesAsthmablessed23No ratings yet
- Case+Study AGN MINEDocument66 pagesCase+Study AGN MINEJm BernardoNo ratings yet
- Pathophysiology (Risk Factors & Symptoms)Document20 pagesPathophysiology (Risk Factors & Symptoms)Ann Michelle TarrobagoNo ratings yet
- Dengue Fever Case StudyDocument5 pagesDengue Fever Case StudyNadine PollescasNo ratings yet
- MDRTB Case StudyDocument35 pagesMDRTB Case StudyFejlean Angelica AntineoNo ratings yet
- Community Health One LinersDocument30 pagesCommunity Health One LinersRatan YadavNo ratings yet
- Dengue 3y1 2Document37 pagesDengue 3y1 2johnmichael008No ratings yet
- Typhoid FeverDocument11 pagesTyphoid FeverjhenvitoNo ratings yet
- Typhoid FeverDocument33 pagesTyphoid FeverBonifacio Diego JrNo ratings yet
- Kidney CancerDocument31 pagesKidney CancerEfren Elico VenguaNo ratings yet
- Tuberculous Meningitis Diagnosis, Treatment and Impact of HIVDocument34 pagesTuberculous Meningitis Diagnosis, Treatment and Impact of HIVLuvi PujiNo ratings yet
- Stomach Cancer Print EditedDocument6 pagesStomach Cancer Print EditedSyazmin KhairuddinNo ratings yet
- Case Study: University of Perpetual HelpDocument30 pagesCase Study: University of Perpetual HelpJanine Kristine P. Dayrit100% (3)
- Measles Koplik's Spots Rash Mucous MembranesDocument17 pagesMeasles Koplik's Spots Rash Mucous MembranesJason AllanNo ratings yet
- Tuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalDocument58 pagesTuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalJoanna RachelNo ratings yet
- PTB Case StudyDocument6 pagesPTB Case StudyTrisha Carolina SottoNo ratings yet
- Leptospirosis: Pauline Teo Siew ChinDocument18 pagesLeptospirosis: Pauline Teo Siew Chinfarmasi_hmNo ratings yet
- Peptic Ulcer DiseaseDocument20 pagesPeptic Ulcer Diseasedr_IstiqlalMiftahulJannahNo ratings yet
- Case Presentation Laryngitis TB 70 TahunDocument21 pagesCase Presentation Laryngitis TB 70 TahunMegan Shanzu100% (1)
- Dengue Fever Signs, Symptoms, and PreventionDocument9 pagesDengue Fever Signs, Symptoms, and PreventionKyla BalboaNo ratings yet
- PericarditisDocument11 pagesPericarditisrbarcellonaNo ratings yet
- Pulmonary Tuberculosis 2016Document17 pagesPulmonary Tuberculosis 2016Nikka Moreen Dagdag100% (1)
- Manila colleges nursing process on Dengue Hemorrhagic FeverDocument14 pagesManila colleges nursing process on Dengue Hemorrhagic FeverShell BalangueNo ratings yet
- TB Case StudyDocument2 pagesTB Case StudyReisabelle LabianoNo ratings yet
- Dengue Breakbone Fever Case StudyDocument53 pagesDengue Breakbone Fever Case StudyLeilani Rodriguez AmpoNo ratings yet
- Signs and Symptoms: Dengue Fever, Also Known As Breakbone Fever, Is ADocument8 pagesSigns and Symptoms: Dengue Fever, Also Known As Breakbone Fever, Is ALutfi AuliaNo ratings yet
- 18 Measles (Rubeola)Document12 pages18 Measles (Rubeola)Sheryl ElitaNo ratings yet
- Chickenpox 1Document7 pagesChickenpox 1Nica Joy CandelarioNo ratings yet
- NTB Control Program ObjectivesDocument46 pagesNTB Control Program ObjectivesJai AdoraNo ratings yet
- Community Acquired PneumoniaDocument28 pagesCommunity Acquired Pneumoniadionisiusvrm100% (1)
- Mumps (Parotitis)Document11 pagesMumps (Parotitis)Indah Lestari100% (1)
- LeptospirosisDocument13 pagesLeptospirosis천사천사No ratings yet
- Typhoid FeverDocument5 pagesTyphoid FeverNaziha InaamNo ratings yet
- MeaslesDocument12 pagesMeaslesyunjung0518100% (3)
- HPV Virus Causes Recurrent Respiratory Papillomatosis in BoyDocument21 pagesHPV Virus Causes Recurrent Respiratory Papillomatosis in BoyDaffa IbnurasyNo ratings yet
- Dengue FeverDocument27 pagesDengue FeverHari Mukti100% (4)
- Case StudyDocument41 pagesCase StudyAubrey Ann FolloscoNo ratings yet
- Ebola Virus DiseaseDocument19 pagesEbola Virus DiseaseAuliani Annisa FebriNo ratings yet
- InfluenzaDocument2 pagesInfluenzajohnndoeeNo ratings yet
- Poststreptococcal GlomerulonephritisDocument19 pagesPoststreptococcal GlomerulonephritisAlex Ismael Catalan CabreraNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Decee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverDocument5 pagesDecee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverJeff Mac Rae RamosNo ratings yet
- The Deadly Mosquito-Borne Dengue Fever VirusDocument52 pagesThe Deadly Mosquito-Borne Dengue Fever VirusnotchNo ratings yet
- Safety Bulletin 35 HOT WORKDocument3 pagesSafety Bulletin 35 HOT WORKTrebor SantosNo ratings yet
- SB 033 Welding and CuttungDocument2 pagesSB 033 Welding and CuttungAl DubNo ratings yet
- FMD-F-11-02.8.2.1 - List of Qualifications For Technical Maintenance PersonnelDocument2 pagesFMD-F-11-02.8.2.1 - List of Qualifications For Technical Maintenance PersonnelTrebor SantosNo ratings yet
- TB BrochureDocument20 pagesTB BrochureTrebor SantosNo ratings yet
- 11 Things That Make Up A Perfect Fire Evacuation DrillDocument2 pages11 Things That Make Up A Perfect Fire Evacuation DrillTrebor SantosNo ratings yet
- Basic Theories of Electrical EstimatingDocument5 pagesBasic Theories of Electrical EstimatingMike AndayaNo ratings yet
- Christmas Decor Safety CertificateDocument2 pagesChristmas Decor Safety CertificateTrebor SantosNo ratings yet
- Safety Bulletin 7 PORTABLE ELECTRICAL EQUIPMENT SAFETYDocument1 pageSafety Bulletin 7 PORTABLE ELECTRICAL EQUIPMENT SAFETYTrebor SantosNo ratings yet
- Safe Working With Flammable SubstancesDocument5 pagesSafe Working With Flammable SubstancesTrebor SantosNo ratings yet
- EHS-G-22 Guidelines On Confined Spaces - Procedure v.3Document13 pagesEHS-G-22 Guidelines On Confined Spaces - Procedure v.3Trebor SantosNo ratings yet
- Hepatitis B BrochureDocument16 pagesHepatitis B BrochureTrebor SantosNo ratings yet
- Hyundai Elevator Preventive Maintenance ProcedureDocument19 pagesHyundai Elevator Preventive Maintenance ProcedureTrebor Santos100% (2)
- Scaffold Safety 2014Document88 pagesScaffold Safety 2014Trebor Santos100% (1)
- Material Handling & Back Safety 26.09.2014Document28 pagesMaterial Handling & Back Safety 26.09.2014Trebor SantosNo ratings yet
- Testing Switchgear Fro Partial Discharge ActivityDocument2 pagesTesting Switchgear Fro Partial Discharge ActivityTrebor SantosNo ratings yet
- FMD-F-11-02.12.2.2 Generator No LoadDocument1 pageFMD-F-11-02.12.2.2 Generator No LoadTrebor SantosNo ratings yet
- Using Ultrasound For High Voltage Insulation Testing - Maintenance TechnologyDocument7 pagesUsing Ultrasound For High Voltage Insulation Testing - Maintenance TechnologyTrebor SantosNo ratings yet
- FMD-F-11-02 12 2 3 - Generator - DailyDocument2 pagesFMD-F-11-02 12 2 3 - Generator - DailyTrebor SantosNo ratings yet
- Nonintrusive Partial Discharge Measurements On High Voltage SwitchgearDocument3 pagesNonintrusive Partial Discharge Measurements On High Voltage SwitchgearTrebor SantosNo ratings yet
- Dengue Fever in The Philippines1Document23 pagesDengue Fever in The Philippines1Nikko MelencionNo ratings yet
- How To Protect Your Organization From Electrical Power OutagesDocument4 pagesHow To Protect Your Organization From Electrical Power OutagesTrebor SantosNo ratings yet
- DiabetesDocument28 pagesDiabetesJohn Paulo Morales100% (1)
- Early Signs of Equipment FailureDocument5 pagesEarly Signs of Equipment FailureTrebor SantosNo ratings yet
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolNo ratings yet
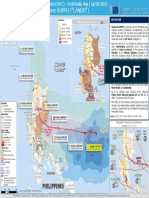
- PHILIPPINES - Tropical Cyclone KOPPU ("LANDO") : LuzonDocument1 pagePHILIPPINES - Tropical Cyclone KOPPU ("LANDO") : LuzonTrebor SantosNo ratings yet
- Compliance Process FlowDocument1 pageCompliance Process FlowTrebor SantosNo ratings yet
- Substation Online Partial Discharge Testing (OLPD) Testing Tech. Update and InfoDocument11 pagesSubstation Online Partial Discharge Testing (OLPD) Testing Tech. Update and InfoTrebor SantosNo ratings yet
- La ThaliliaDocument1 pageLa ThaliliaTrebor SantosNo ratings yet
- ASTMH Exam Brochure 18 FNLDocument17 pagesASTMH Exam Brochure 18 FNLNgô Khánh HuyềnNo ratings yet
- (2021) Critical Review and Research Needs of Ozone Applications Related To Virus Inactivation Potential Implications For SARS CoV 2Document20 pages(2021) Critical Review and Research Needs of Ozone Applications Related To Virus Inactivation Potential Implications For SARS CoV 2Vu TranNo ratings yet
- Mapping The Antigenic and Genetic Evolution of in Uenza VirusDocument7 pagesMapping The Antigenic and Genetic Evolution of in Uenza Virusaleisha97No ratings yet
- Case Study PPT - PDF HIV With Opportunistic Infection - Madayag March 2023Document71 pagesCase Study PPT - PDF HIV With Opportunistic Infection - Madayag March 2023Rasheda PickettNo ratings yet
- Understanding HIV/AIDSDocument2 pagesUnderstanding HIV/AIDSMbiatat BrandonNo ratings yet
- Persuasive Speech on Importance of COVID-19 VaccinationDocument2 pagesPersuasive Speech on Importance of COVID-19 VaccinationRonn ArtajoNo ratings yet
- Byju's Magazine (PDFDrive)Document23 pagesByju's Magazine (PDFDrive)iocsachinNo ratings yet
- Antibioticresistance PowerpointDocument51 pagesAntibioticresistance PowerpointOdy100% (1)
- Virology Summary: Viruses Structure, Replication Cycle & ClassificationDocument3 pagesVirology Summary: Viruses Structure, Replication Cycle & ClassificationvictorNo ratings yet
- BioChemistry Syllabus and MQPs 08012018Document33 pagesBioChemistry Syllabus and MQPs 08012018rupaNo ratings yet
- The Special Features of Alpha-Monolaurin To Support Poultry PerformanceDocument1 pageThe Special Features of Alpha-Monolaurin To Support Poultry PerformanceDrivailaNo ratings yet
- Week 1 cb1131 NotesDocument24 pagesWeek 1 cb1131 NotesTanisha ChowdharyNo ratings yet
- Infectious Disease in An Era of GlobalDocument13 pagesInfectious Disease in An Era of Globalsebastian herreraNo ratings yet
- Myco Viro InterSem2022Document9 pagesMyco Viro InterSem2022Arienda RKNo ratings yet
- History of Polio-1Document21 pagesHistory of Polio-1world photocopyNo ratings yet
- Grade 10 Health UNIT 3 Health Trends Issues and Concern Global LevelDocument7 pagesGrade 10 Health UNIT 3 Health Trends Issues and Concern Global LevelJeffer Balilo100% (1)
- Broncho VaxomDocument18 pagesBroncho VaxomSABUESO FINANCIERONo ratings yet
- MSC Biotechnology Syllabus FINALDocument53 pagesMSC Biotechnology Syllabus FINALdeepakNo ratings yet
- Microbiology Topics: Hepatitis B Infection Section 1Document16 pagesMicrobiology Topics: Hepatitis B Infection Section 1Zeidan MohammadNo ratings yet
- Bes More On MiasmDocument16 pagesBes More On MiasmSatyendra RawatNo ratings yet
- INTEGRIS COVID19Interpreting COVID19 Test Results7720Document2 pagesINTEGRIS COVID19Interpreting COVID19 Test Results7720nellyNo ratings yet
- DD FeverDocument9 pagesDD FeverAnisa WahyuniartiNo ratings yet
- Song 2021Document28 pagesSong 2021Supu VeeturiNo ratings yet
- The Etiology of Glomerulonephritis: Roles of Infection and AutoimmunityDocument10 pagesThe Etiology of Glomerulonephritis: Roles of Infection and AutoimmunityCarlos DominguezNo ratings yet
- Dengue FeverDocument8 pagesDengue Feverramoli1988No ratings yet
- Bacterial Meningitis Symptoms, Causes, Diagnosis and TreatmentDocument30 pagesBacterial Meningitis Symptoms, Causes, Diagnosis and TreatmentFaris Alarshani100% (1)