You might also like
- Assessing the Abdomen: 4 Quadrants and 9 RegionsDocument54 pagesAssessing the Abdomen: 4 Quadrants and 9 RegionsWilma Acorin OrillinedaNo ratings yet
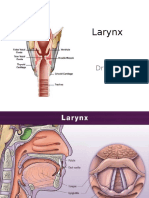
- The Larynx: Structure, Function and Clinical NotesDocument34 pagesThe Larynx: Structure, Function and Clinical NotesJojo Ryelcius100% (1)
- True Undescened TestesDocument42 pagesTrue Undescened TestesSahirNo ratings yet
- Ovaries & AdnexaeDocument124 pagesOvaries & AdnexaeabafzNo ratings yet
- Abdominal HysterectomyDocument23 pagesAbdominal Hysterectomytata marethaNo ratings yet
- 3-Inguinal Canal PDFDocument58 pages3-Inguinal Canal PDFN A0% (1)
- Ectopic PregnancyDocument14 pagesEctopic PregnancytaufiqNo ratings yet
- Section 2 The Female Genital Organs: Gonad - Conveying Ducts - Accessory GlandsDocument29 pagesSection 2 The Female Genital Organs: Gonad - Conveying Ducts - Accessory Glandssomebody_maNo ratings yet
- HypoxiaDocument21 pagesHypoxiaJojo RyelciusNo ratings yet
- 1 Bony PelvisDocument50 pages1 Bony PelvisNicole NgoNo ratings yet
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- Get A Good Nights SleepDocument35 pagesGet A Good Nights SleepGeorge Sebastian AntonyNo ratings yet
- Cardiac Disease in PregnancyDocument28 pagesCardiac Disease in PregnancyviharadewiNo ratings yet
- Blood Transfusion MCQDocument6 pagesBlood Transfusion MCQShrestha Anjiv95% (58)
- Spinal Cord TumorsDocument23 pagesSpinal Cord TumorsTahleel AltafNo ratings yet
- Carcinoma of The Breast - Bailey & LoveDocument5 pagesCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Development of MesentryDocument28 pagesDevelopment of MesentryimmmiNo ratings yet
- 1GS Cell PPT 2018Document73 pages1GS Cell PPT 2018pixiedustNo ratings yet
- 8384 ST PDFDocument20 pages8384 ST PDFJohn Dave Francisco100% (1)
- Congenital Anomalies of Urinary BladderDocument102 pagesCongenital Anomalies of Urinary Bladdernancy voraNo ratings yet
- Gallbladder Cancer Treatment and PrognosisDocument61 pagesGallbladder Cancer Treatment and PrognosisZaki DhiifNo ratings yet
- Bladder Outlet Obstruction in Children PDFDocument64 pagesBladder Outlet Obstruction in Children PDFalaaNo ratings yet
- Digestive System Anatomy and Physiology - NurseslabsDocument33 pagesDigestive System Anatomy and Physiology - NurseslabsMari FeNo ratings yet
- Upper Respiratory Tract AnatomyDocument61 pagesUpper Respiratory Tract Anatomyيحيى اسماعيل الجميليNo ratings yet
- Early Pregnancy Bleeding Causes and TypesDocument51 pagesEarly Pregnancy Bleeding Causes and TypesMesk Banat100% (2)
- CSFDocument40 pagesCSFDrNaveen Singh Rajpurohit KaduNo ratings yet
- Hernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsDocument43 pagesHernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsFobin VargheseNo ratings yet
- Pelvic Organ Prolapse GuideDocument48 pagesPelvic Organ Prolapse GuideKerod AbebeNo ratings yet
- Billiary SystemDocument60 pagesBilliary SystemDONALD UNASHENo ratings yet
- Rectum & Anal CanalDocument14 pagesRectum & Anal CanalLisa DentonNo ratings yet
- Anorectal Anatomy & Surgical ManagementDocument164 pagesAnorectal Anatomy & Surgical Managementsgod34No ratings yet
- Ultrasound Spleen GuideDocument16 pagesUltrasound Spleen GuideJohn Andre RamosNo ratings yet
- Tumor of Small IntestineDocument27 pagesTumor of Small IntestinePRUTHVI RAJ P SNo ratings yet
- Medical Imaging TechniquesDocument96 pagesMedical Imaging TechniquesNazia WasimNo ratings yet
- Disordered of The Breast: Abdelkarim BarqawiDocument63 pagesDisordered of The Breast: Abdelkarim BarqawiRazan HaimounyNo ratings yet
- Ilovepdf MergedDocument457 pagesIlovepdf MergedMar LoyolaNo ratings yet
- A Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressDocument299 pagesA Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressHamza Khan100% (1)
- Liver Functions Guide: Bile, Blood Filtration & MetabolismDocument60 pagesLiver Functions Guide: Bile, Blood Filtration & MetabolismqueenuagNo ratings yet
- Amoebiasis Case PresentationDocument28 pagesAmoebiasis Case Presentationjan micah100% (1)
- Cytopathology of Neuroendocrine Neoplasia - Color Atlas and TextDocument411 pagesCytopathology of Neuroendocrine Neoplasia - Color Atlas and TextIsabella CrăciunNo ratings yet
- Breech Presentation 1Document33 pagesBreech Presentation 1Cristina StanleeNo ratings yet
- CV-Prof-MulyadiDocument69 pagesCV-Prof-MulyadityesNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Hisprung DiseaseDocument12 pagesHisprung DiseaseEky Madyaning NastitiNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument28 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Liver and Biliary System: DR Anil Chaudhary Associate Professor PhysiologyDocument31 pagesLiver and Biliary System: DR Anil Chaudhary Associate Professor Physiologylion2chNo ratings yet
- Female PelvisDocument18 pagesFemale Pelvisveegeer100% (6)
- Chapter 2 Maternal AnatomyDocument9 pagesChapter 2 Maternal AnatomyRem Alfelor100% (2)
- GYNE UltrasoundgyneDocument11 pagesGYNE UltrasoundgyneMara AbantoNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- Anatomy Physiology PregnancyDocument45 pagesAnatomy Physiology PregnancyFilbertaNo ratings yet
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 pagesObstetric Anal Sphincter Injury (OASIS) - UpToDateErickNo ratings yet
- Testicular TorsionDocument12 pagesTesticular TorsionlicutNo ratings yet
- Breech Presentation ManagementDocument16 pagesBreech Presentation Managementhussain AltaherNo ratings yet
- Anatomy of the female bony pelvisDocument16 pagesAnatomy of the female bony pelvismichael0202No ratings yet
- Histology Lower GIT Microscopic Features Small Large IntestineDocument27 pagesHistology Lower GIT Microscopic Features Small Large IntestineArwa100% (2)
- Intestinal Atresia and StenosisDocument7 pagesIntestinal Atresia and StenosisMichael NafarinNo ratings yet
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- 1 InroductionDocument44 pages1 Inroductiondemeke andebetNo ratings yet
- SoTM StaplingDocument20 pagesSoTM StaplingIndrawan Buleth100% (1)
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- Mal RotationDocument13 pagesMal RotationkavyarkrnagarNo ratings yet
- Pelvic BoneDocument15 pagesPelvic BoneYoanneveline TanakNo ratings yet
- Per Rectal Bleeding CompiledDocument33 pagesPer Rectal Bleeding CompiledRajhmuniran Kandasamy100% (1)
- Properties of Cardiac Muscle PDFDocument38 pagesProperties of Cardiac Muscle PDFZaid RazaliNo ratings yet
- Ventric Ul Omega LyDocument40 pagesVentric Ul Omega LyErliana FaniNo ratings yet
- Pathophysiology of Breast CancerDocument8 pagesPathophysiology of Breast CancerNicole Villanueva, BSN - Level 3ANo ratings yet
- Direct Inguinal Hernia GuideDocument11 pagesDirect Inguinal Hernia GuideRizka JamaraNo ratings yet
- BREAST Development TSADocument62 pagesBREAST Development TSAshirley_ling_15No ratings yet
- Omega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenDocument10 pagesOmega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenJojo RyelciusNo ratings yet
- Klasifikasi BMI & Profil LipidDocument1 pageKlasifikasi BMI & Profil LipidOkky Rizka SesarinaNo ratings yet
- Breast FeedingDocument11 pagesBreast FeedingJojo RyelciusNo ratings yet
- Struktur Clinical ReasoningDocument15 pagesStruktur Clinical ReasoningJojo RyelciusNo ratings yet
- Melanoma and Other Skin Cancers: What You Need To Know AboutDocument59 pagesMelanoma and Other Skin Cancers: What You Need To Know AboutkikiNo ratings yet
- Clinical ReasoningDocument15 pagesClinical ReasoningJojo RyelciusNo ratings yet
- Omega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenDocument10 pagesOmega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenJojo RyelciusNo ratings yet
- Stres Cairan Dan SuhuDocument94 pagesStres Cairan Dan SuhuJojo RyelciusNo ratings yet
- Skenario C Blok 10 FixDocument32 pagesSkenario C Blok 10 FixJojo RyelciusNo ratings yet
- 5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44Document37 pages5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44gothai sivapragasamNo ratings yet
- Female Reproductive AnatomydDocument7 pagesFemale Reproductive AnatomydOneda Ganbatte' KudasaiNo ratings yet
- 8.2 # Human Digestive SystemDocument5 pages8.2 # Human Digestive SystemSara Nadeem KhanNo ratings yet
- JaundiceDocument6 pagesJaundiceKesyaNo ratings yet
- Exercise Therapy Old PapersDocument8 pagesExercise Therapy Old PapersJust ChepthunnaNo ratings yet
- Hkcee Biology - 4.6 Transport in Humans - P.1Document17 pagesHkcee Biology - 4.6 Transport in Humans - P.1ミーチェルNo ratings yet
- Anatomy and Physiology of the Male and Female Reproductive SystemsDocument55 pagesAnatomy and Physiology of the Male and Female Reproductive SystemsJeffrey Roy Adlawan LopezNo ratings yet
- DentinDocument89 pagesDentinDr Zadeno kithanNo ratings yet
- Plant and Animal Organ System and Their FunctionsDocument78 pagesPlant and Animal Organ System and Their FunctionssannsannNo ratings yet
- Brain Review JeopardyDocument51 pagesBrain Review Jeopardyapi-261267976No ratings yet
- Suggested Answers To Exercise, Reading To Learn and Cross-Topic ExerciseDocument19 pagesSuggested Answers To Exercise, Reading To Learn and Cross-Topic ExerciseBernardNo ratings yet
- Bone and muscle structure, function, and developmentDocument6 pagesBone and muscle structure, function, and developmentLuna ScorpiusNo ratings yet
- Pathology: HematologyDocument1 pagePathology: HematologyMubashar AliNo ratings yet
- Grade 4 Summative Test for Science and Music Covers Key ConceptsDocument2 pagesGrade 4 Summative Test for Science and Music Covers Key ConceptsCristita Macaranas Vigo100% (1)
- RADIOLOGY ASPECT OF EXTRA PULMONARY TUBERCULOSISDocument45 pagesRADIOLOGY ASPECT OF EXTRA PULMONARY TUBERCULOSISAndre F SusantioNo ratings yet
- Foetal Membrane and Amniotic Fluid FunctionsDocument10 pagesFoetal Membrane and Amniotic Fluid FunctionsN. SivaNo ratings yet
- Male Reproductive System CanvaDocument35 pagesMale Reproductive System CanvaDex VargasNo ratings yet
- Cancer Cytopathology - 2017 - La Fortune - Improvements in Cell Block Processing The Cell Gel MethodDocument10 pagesCancer Cytopathology - 2017 - La Fortune - Improvements in Cell Block Processing The Cell Gel MethodVlad TomaNo ratings yet
- Comparing Male and Female Reproductive SystemsDocument11 pagesComparing Male and Female Reproductive SystemsRia Biong TaripeNo ratings yet
- Hyperleukocytosis and leukostasis in hematologic malignanciesDocument13 pagesHyperleukocytosis and leukostasis in hematologic malignanciesIGD RSKDNo ratings yet
- 29.3 Book BioDocument4 pages29.3 Book BioBadawi ashrafNo ratings yet