You might also like
- Letter To The President of Indonesia COVID-19 and Tobacco Smoking-Call To Action by 42 Prominent Organizations English Version April 15, 2020Document6 pagesLetter To The President of Indonesia COVID-19 and Tobacco Smoking-Call To Action by 42 Prominent Organizations English Version April 15, 2020bobbyramakant100% (1)
- Prepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Document53 pagesPrepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Mir JavidNo ratings yet
- International Journal of Infectious DiseasesDocument4 pagesInternational Journal of Infectious DiseasesPedro MalikNo ratings yet
- Linezolid To Treat MDR-/XDR-tuberculosis: Available Evidence and Future ScenariosDocument5 pagesLinezolid To Treat MDR-/XDR-tuberculosis: Available Evidence and Future ScenariosNop PiromNo ratings yet
- What Is Multidrug-Resistant Tuberculosis (MDR-TB) and How Do We Control It?Document2 pagesWhat Is Multidrug-Resistant Tuberculosis (MDR-TB) and How Do We Control It?Dvica SarahNo ratings yet
- WHO Bulletin 2005Document10 pagesWHO Bulletin 2005ajh2675No ratings yet
- Management of Patients With Multidrug-Resistant TuberculosisDocument19 pagesManagement of Patients With Multidrug-Resistant TuberculosisCristopher OchoaNo ratings yet
- Burden of Tuberculosis - Combating Drug Resistance: EditorialDocument3 pagesBurden of Tuberculosis - Combating Drug Resistance: EditorialmominamalikNo ratings yet
- Multidrug-Resistant Tuberculosis (MDR-TB) : 2012 UpdateDocument2 pagesMultidrug-Resistant Tuberculosis (MDR-TB) : 2012 UpdateRobert MontgomeryNo ratings yet
- Anti-Infectives Drug Advisory Committee MeetingDocument253 pagesAnti-Infectives Drug Advisory Committee MeetingbellamajNo ratings yet
- TheUnion DR TB GuideDocument2 pagesTheUnion DR TB GuideDhani KurniawanNo ratings yet
- BY Dr. Tahmina AzharDocument71 pagesBY Dr. Tahmina Azharscribdnotes123No ratings yet
- JurnalDocument4 pagesJurnalAnonymous pfHZusnNo ratings yet
- jh08003 PDFDocument8 pagesjh08003 PDFkiranaNo ratings yet
- TB Burden and Treatment Guidelines: DR Malgosia Grzemska Global TB Programme, WHO/HQDocument25 pagesTB Burden and Treatment Guidelines: DR Malgosia Grzemska Global TB Programme, WHO/HQSuresh ShresthaNo ratings yet
- MDR TB FactsheetDocument2 pagesMDR TB FactsheetfaradillaNo ratings yet
- Multi Drug ResistenDocument2 pagesMulti Drug ResistenNurul W.ANo ratings yet
- Molecular AnalysisDocument29 pagesMolecular AnalysisBaranishankarNo ratings yet
- MDR-TB Treatment As Prevention: The Projected Population-Level Impact of Expanded Treatment For Multidrug-Resistant TuberculosisDocument16 pagesMDR-TB Treatment As Prevention: The Projected Population-Level Impact of Expanded Treatment For Multidrug-Resistant TuberculosisSorina ElenaNo ratings yet
- JH 08003Document8 pagesJH 08003Nur Afni PonsengNo ratings yet
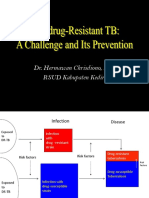
- Dr. Hermawan Chrisdiono, SP.P RSUD Kabupaten KediriDocument48 pagesDr. Hermawan Chrisdiono, SP.P RSUD Kabupaten KediribotolkecapNo ratings yet
- Multidrug-Resistant Tuberculosis (MDR-TB) Is Defined As TB That Is Resistant To BothDocument4 pagesMultidrug-Resistant Tuberculosis (MDR-TB) Is Defined As TB That Is Resistant To Bothsanny_sundariNo ratings yet
- The Revised National Tuberculosis Control ProgrammeDocument2 pagesThe Revised National Tuberculosis Control ProgrammesuryaslideNo ratings yet
- Tuberculosis: An OverviewDocument45 pagesTuberculosis: An OverviewaNo ratings yet
- Drug Resistance of TBDocument17 pagesDrug Resistance of TBGaurav Sharma100% (1)
- Mjhid 6 1 E2014070Document8 pagesMjhid 6 1 E2014070Khoiril AnwarNo ratings yet
- Epidemiology of Tuberculosis - UpToDateDocument33 pagesEpidemiology of Tuberculosis - UpToDateCentro de salud El quincheNo ratings yet
- Contemporary Data On TB Epidemiology by Nwokotubo Beulah 2Document26 pagesContemporary Data On TB Epidemiology by Nwokotubo Beulah 2Beulah AlexNo ratings yet
- The WHO Strategy For TB Control and EliminationDocument12 pagesThe WHO Strategy For TB Control and EliminationAdel HamadaNo ratings yet
- TRT2017 4920209Document12 pagesTRT2017 4920209ADVOCATE ASHUTOSH SHARMANo ratings yet
- Multidrug-Resistant Tuberculosis in Uzbekistan: Results of A Nationwide Survey, 2010 To 2011Document12 pagesMultidrug-Resistant Tuberculosis in Uzbekistan: Results of A Nationwide Survey, 2010 To 2011IsoqjonivichNo ratings yet
- Tuberculosis:Development of New Drugs and Treatment RegimensDocument10 pagesTuberculosis:Development of New Drugs and Treatment RegimensMedylin DualloNo ratings yet
- Tuberculosis: Infection and TransmissionDocument7 pagesTuberculosis: Infection and TransmissionMonica AgapitoNo ratings yet
- What, Where, How and Action StepsDocument11 pagesWhat, Where, How and Action StepslaviganeNo ratings yet
- Recent Developments in The Diagnosis and Management of TuberculosisDocument8 pagesRecent Developments in The Diagnosis and Management of TuberculosisRhahahaNo ratings yet
- The Global Alliance For Tuberculosis Drug DevelopmentDocument9 pagesThe Global Alliance For Tuberculosis Drug DevelopmentRichard WooliteNo ratings yet
- Tuberculosis: Forgotten But Not GoneDocument65 pagesTuberculosis: Forgotten But Not GoneNational Press FoundationNo ratings yet
- Tuberculosis: WHO Global Tuberculosis Report 2014Document2 pagesTuberculosis: WHO Global Tuberculosis Report 2014blueicelandNo ratings yet
- 411 TB FactsheetDocument54 pages411 TB FactsheetKimberly SebekNo ratings yet
- Who Cds CPC TB 99.270Document39 pagesWho Cds CPC TB 99.270Mary Rose Pantinople CejuelaNo ratings yet
- Management of HIV-associated Tuberculosis in Resource-Limited Settings: A State-Of-The-Art ReviewDocument16 pagesManagement of HIV-associated Tuberculosis in Resource-Limited Settings: A State-Of-The-Art Reviewbarokahgroup groupNo ratings yet
- 1.TB - Prevention - TPT OnlineDocument25 pages1.TB - Prevention - TPT Onlinehumairaismail3No ratings yet
- TBC and VihDocument12 pagesTBC and VihCynthia O. CórdovaNo ratings yet
- Minireview: New Drugs Against Tuberculosis: Problems, Progress, and Evaluation of Agents in Clinical DevelopmentDocument14 pagesMinireview: New Drugs Against Tuberculosis: Problems, Progress, and Evaluation of Agents in Clinical DevelopmentcgandarelaNo ratings yet
- Multi-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyDocument3 pagesMulti-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyJhemar Handa JulhamidNo ratings yet
- 00010-2015 Full PDFDocument15 pages00010-2015 Full PDFChristabella Natalia WijayaNo ratings yet
- Akurit 4 TBDocument14 pagesAkurit 4 TBNicolloNo ratings yet
- MDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDDocument33 pagesMDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- WHO - Anti TB Treatment For ChildrenDocument7 pagesWHO - Anti TB Treatment For ChildrenSistya RestuningrumNo ratings yet
- Mutidrug Resistant TuberculosisDocument2 pagesMutidrug Resistant Tuberculosistummalapalli venkateswara raoNo ratings yet
- TB-Guidelines 2019 Final - 200619Document105 pagesTB-Guidelines 2019 Final - 200619Kalash SinghalNo ratings yet
- Baluchestan ProvinceDocument9 pagesBaluchestan ProvinceVincentius Michael WilliantoNo ratings yet
- Materi TPT WHO Recommendation 22 Juli 2021 - DR - Regina WHODocument44 pagesMateri TPT WHO Recommendation 22 Juli 2021 - DR - Regina WHOvhiiaNo ratings yet
- Diagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanDocument20 pagesDiagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanHermanto QuedarusmanNo ratings yet
- Latent TB Infection Provider GuideDocument17 pagesLatent TB Infection Provider GuideRivani KurniawanNo ratings yet
- Tuberculosis: Forgotten But Not Gone (Lee B. Reichman, M.D., M.P.H.)Document38 pagesTuberculosis: Forgotten But Not Gone (Lee B. Reichman, M.D., M.P.H.)National Press FoundationNo ratings yet
- NTEP or RNTCP (Community Health Nursing)Document37 pagesNTEP or RNTCP (Community Health Nursing)Ankita ShaluNo ratings yet
- 1201 Sanchez Padilla High Prevalence of Multidrug Resistant Tuberculosis Swaziland 2009 2010 Emerging Infectious Diseases 18 1Document9 pages1201 Sanchez Padilla High Prevalence of Multidrug Resistant Tuberculosis Swaziland 2009 2010 Emerging Infectious Diseases 18 1dewi ayu wulandariNo ratings yet
- Chest: Relevance of Latent TB Infection in Areas of High TB PrevalenceDocument13 pagesChest: Relevance of Latent TB Infection in Areas of High TB PrevalenceAfifah RizkianaNo ratings yet
- APCRSHR10 Virtual: Abstract Presentation by SM Shaikat (Ensuring Youth Voices by Establishing Sustainable National Platform For SRHR)Document9 pagesAPCRSHR10 Virtual: Abstract Presentation by SM Shaikat (Ensuring Youth Voices by Establishing Sustainable National Platform For SRHR)bobbyramakantNo ratings yet
- Abstract Presentation: Olanike Adedeji (Roadmap To Achieving Zero Unmet Need in The Pacific)Document27 pagesAbstract Presentation: Olanike Adedeji (Roadmap To Achieving Zero Unmet Need in The Pacific)bobbyramakantNo ratings yet
- Abstract Presentation: Anna Ravendran and Kate Burry of Family Planning New Zealand (SRHR in Rural Vanuatu: Knowledge, Access and Barriers)Document14 pagesAbstract Presentation: Anna Ravendran and Kate Burry of Family Planning New Zealand (SRHR in Rural Vanuatu: Knowledge, Access and Barriers)bobbyramakantNo ratings yet
- Plenary Presentation: Karen Hill (SRHR in The Pacific: Strategic Approach)Document18 pagesPlenary Presentation: Karen Hill (SRHR in The Pacific: Strategic Approach)bobbyramakantNo ratings yet
- Access To Male Family Planning Methods in Timor-Leste - Preliminary Findings From A Qualitative Participatory Research ProjectDocument14 pagesAccess To Male Family Planning Methods in Timor-Leste - Preliminary Findings From A Qualitative Participatory Research ProjectbobbyramakantNo ratings yet
- The Cost of "Growing Up"Document15 pagesThe Cost of "Growing Up"bobbyramakantNo ratings yet
- Leveraging Sport To Improve Perceptions of Violence and Sexual and Reproductive Health and Rights For AdolescentsDocument12 pagesLeveraging Sport To Improve Perceptions of Violence and Sexual and Reproductive Health and Rights For AdolescentsbobbyramakantNo ratings yet
- Opportunities For Strengthening Sexual Health Education in SchoolsDocument13 pagesOpportunities For Strengthening Sexual Health Education in SchoolsbobbyramakantNo ratings yet
- Needs of Comprehensive Sexuality Education (Cse) of Students in Thai Nguyen University (Tnu), VietnamDocument15 pagesNeeds of Comprehensive Sexuality Education (Cse) of Students in Thai Nguyen University (Tnu), VietnambobbyramakantNo ratings yet
- Shreya Rawal and Durgesh Nandan Yadav Poster On SolidarityDocument1 pageShreya Rawal and Durgesh Nandan Yadav Poster On SolidaritybobbyramakantNo ratings yet
- Abstract presentation: Rayner Kay Jin Tan (experienced homophobia and suicide ideation in young gay, bisexual, and queer men: Exploring the mediating role of depressive symptoms, self-esteem, and outness in the Pink Carpet Y Cohort Study)Document24 pagesAbstract presentation: Rayner Kay Jin Tan (experienced homophobia and suicide ideation in young gay, bisexual, and queer men: Exploring the mediating role of depressive symptoms, self-esteem, and outness in the Pink Carpet Y Cohort Study)bobbyramakantNo ratings yet
- DR Gilada - Intervention Application Before Hon. SCI - FinalDocument18 pagesDR Gilada - Intervention Application Before Hon. SCI - FinalbobbyramakantNo ratings yet
- Prof Caroline Homer's Plenary Presentation at #APCRSHR10 Virtual (29 June 2020)Document18 pagesProf Caroline Homer's Plenary Presentation at #APCRSHR10 Virtual (29 June 2020)bobbyramakantNo ratings yet
- DR Kerri Viney's Presentation in UHC Day Webinar On 12th December 2017Document18 pagesDR Kerri Viney's Presentation in UHC Day Webinar On 12th December 2017bobbyramakant100% (1)
- "Will The World Be The Same Again?" Questions Shashwat ChourasiyaDocument1 page"Will The World Be The Same Again?" Questions Shashwat ChourasiyabobbyramakantNo ratings yet
- ARROW for Change - Intersections: The Politicisation of Religion and Sexual and Reproductive Health and Rights (Hindi/ हिंदी translation)Document48 pagesARROW for Change - Intersections: The Politicisation of Religion and Sexual and Reproductive Health and Rights (Hindi/ हिंदी translation)bobbyramakantNo ratings yet
- The Leader Lies in You (Success Stories of Women Farmers in UP, India)Document68 pagesThe Leader Lies in You (Success Stories of Women Farmers in UP, India)bobbyramakantNo ratings yet
- Dean PresentationDocument33 pagesDean PresentationbobbyramakantNo ratings yet
- Health Experts Meet Telangana Governor DR Tamilisai Soundararajan: Memorandum Submitted To Telangana GovernorDocument2 pagesHealth Experts Meet Telangana Governor DR Tamilisai Soundararajan: Memorandum Submitted To Telangana GovernorbobbyramakantNo ratings yet
- DR Shivani Sharma Pandey's Slides On Challenges With Autistic ChildrenDocument6 pagesDR Shivani Sharma Pandey's Slides On Challenges With Autistic ChildrenbobbyramakantNo ratings yet
- Presentation of DR Linda-Gail Bekker in World AIDS Day Webinar On 28/11Document41 pagesPresentation of DR Linda-Gail Bekker in World AIDS Day Webinar On 28/11bobbyramakantNo ratings yet
- Presentation of Gini Williams For Universal Health Coverage Day Webinar #UHC 2017Document6 pagesPresentation of Gini Williams For Universal Health Coverage Day Webinar #UHC 2017bobbyramakantNo ratings yet
- Paula I Fujiwara PresentationDocument16 pagesPaula I Fujiwara PresentationbobbyramakantNo ratings yet
- Presentation of DR Archana Trivedi, One of Co-Authors of Study On Mhealth and TBDocument11 pagesPresentation of DR Archana Trivedi, One of Co-Authors of Study On Mhealth and TBbobbyramakantNo ratings yet
- DR Nguyen Viet Nhung's Presentation in #endTB WebinarDocument10 pagesDR Nguyen Viet Nhung's Presentation in #endTB WebinarbobbyramakantNo ratings yet
- Presentation of DR Paula I Fujiwara of The Union in 2017 World Lung Day WebinarDocument16 pagesPresentation of DR Paula I Fujiwara of The Union in 2017 World Lung Day WebinarbobbyramakantNo ratings yet
- Presentation of DR Dean E Schraufnagel, Director, FIRS in 2017 World Lung Day WebinarDocument33 pagesPresentation of DR Dean E Schraufnagel, Director, FIRS in 2017 World Lung Day WebinarbobbyramakantNo ratings yet
- Kavita Ayyagari's Presentation in #endTB WebinarDocument17 pagesKavita Ayyagari's Presentation in #endTB WebinarbobbyramakantNo ratings yet
- DR Enos Masini's Presentation On Inter-Sectoral Response To Increase Access To Child-Friendly TB Meds: SDM Health Justice Lecture, July 2017Document19 pagesDR Enos Masini's Presentation On Inter-Sectoral Response To Increase Access To Child-Friendly TB Meds: SDM Health Justice Lecture, July 2017bobbyramakantNo ratings yet