You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mini Project 1 - 1Document9 pagesMini Project 1 - 1Sameer BaraNo ratings yet
- Pref - 2 - Grammar 1.2 - Revisión Del IntentoDocument2 pagesPref - 2 - Grammar 1.2 - Revisión Del IntentoJuan M. Suarez ArevaloNo ratings yet
- Tsel Manual ThermoselDocument25 pagesTsel Manual ThermoselPedro AlvelaisNo ratings yet
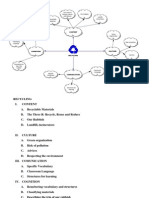
- Recycling Mind MapDocument2 pagesRecycling Mind Mapmsole124100% (1)
- How To Eat WellDocument68 pagesHow To Eat WelleledidiNo ratings yet
- Mullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorDocument15 pagesMullā Ṣadrā and Causation - Rethinking A Problem in Later Islamic Philosophy AuthorKadag LhundrupNo ratings yet
- Food Biotechnology in Ethical PerspectiveDocument340 pagesFood Biotechnology in Ethical Perspectivemojtaba2500100% (2)
- Marvell 88F37xx Product Brief 20160830Document2 pagesMarvell 88F37xx Product Brief 20160830Sassy FiverNo ratings yet
- 40 RT-flex Control-System Rev01Document68 pages40 RT-flex Control-System Rev01Mayvon Botelho100% (2)
- Mini-Case 1 Ppe AnswerDocument11 pagesMini-Case 1 Ppe Answeryu choong100% (2)
- Orofacial Complex: Form and FunctionDocument34 pagesOrofacial Complex: Form and FunctionAyushi Goel100% (1)
- DNA Mutation and Its Effect To An Individual (w5)Document6 pagesDNA Mutation and Its Effect To An Individual (w5)Cold CoockiesNo ratings yet
- Upaam 1135891 202105060749199700Document18 pagesUpaam 1135891 202105060749199700Kartik KapoorNo ratings yet
- Trends in FoodDocument3 pagesTrends in FoodAliNo ratings yet
- PTP S3Document8 pagesPTP S3Yongyin SHENGNo ratings yet
- Salapare Et Al 2015 ZambalesDocument12 pagesSalapare Et Al 2015 ZambalesTiqfar AhmadjayadiNo ratings yet
- Statistics and Probability Module 3Document3 pagesStatistics and Probability Module 3Eftychia LeegleeNo ratings yet
- American University of BeirutDocument21 pagesAmerican University of BeirutWomens Program AssosciationNo ratings yet
- Industrial Internet of Things: Presented To-Presented byDocument18 pagesIndustrial Internet of Things: Presented To-Presented byGaurav RaturiNo ratings yet
- ANS: (2.59807m/s2 Horizontal) (1.5m/s2 Vertical) (12.93725 Degree Angle That The Water Surface Makes With The Horizontal)Document5 pagesANS: (2.59807m/s2 Horizontal) (1.5m/s2 Vertical) (12.93725 Degree Angle That The Water Surface Makes With The Horizontal)Lolly UmaliNo ratings yet
- Modern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaDocument2 pagesModern Myth and Magical Face Shifting Technology in Girish Karnad Hayavadana and NagamandalaKumar KumarNo ratings yet
- Resumen C37 010 Aplicacion de Breaker Disenados IC Simetrica PDFDocument9 pagesResumen C37 010 Aplicacion de Breaker Disenados IC Simetrica PDFglendathais100% (1)
- AR BuildingDocument819 pagesAR BuildingShithin KrishnanNo ratings yet
- Firestone & Scholl - Cognition Does Not Affect Perception, Evaluating Evidence For Top-Down EffectsDocument77 pagesFirestone & Scholl - Cognition Does Not Affect Perception, Evaluating Evidence For Top-Down EffectsRed JohnNo ratings yet
- QuantAssay Software Manual 11-Mar-2019Document51 pagesQuantAssay Software Manual 11-Mar-2019LykasNo ratings yet
- Chapter 10 - The Mature ErythrocyteDocument55 pagesChapter 10 - The Mature ErythrocyteSultan AlexandruNo ratings yet
- All About PlantsDocument14 pagesAll About Plantsapi-234860390No ratings yet
- Energy Transfer in Cell During Exercise and Oxygen Metabolism and Transport - PalakDocument85 pagesEnergy Transfer in Cell During Exercise and Oxygen Metabolism and Transport - Palakpalooo4No ratings yet
- Full Download Short Term Financial Management 3rd Edition Maness Test BankDocument35 pagesFull Download Short Term Financial Management 3rd Edition Maness Test Bankcimanfavoriw100% (31)
- Manual Nice9000v A04Document151 pagesManual Nice9000v A04hoang tamNo ratings yet