You might also like
- Secondary TuberculosisDocument11 pagesSecondary TuberculosisSarvess MuniandyNo ratings yet
- Giardiasis PDFDocument14 pagesGiardiasis PDFSaad Motawéa0% (1)
- Dengue Fever and Some Case Reports From Delhi Govt. Homoeopathic DispensariesDocument7 pagesDengue Fever and Some Case Reports From Delhi Govt. Homoeopathic DispensariesHomoeopathic PulseNo ratings yet
- Pheochromocytoma and HomoeopathyDocument13 pagesPheochromocytoma and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- CCH Organon SyllabusDocument6 pagesCCH Organon SyllabusMadiha SheikhNo ratings yet
- Aethusa CynapiumDocument4 pagesAethusa CynapiumnitkolNo ratings yet
- A Weekly Journal Club PresentationDocument61 pagesA Weekly Journal Club PresentationSharyKrishnaNo ratings yet
- Topical Drug DeliveryDocument21 pagesTopical Drug DeliveryhappyNo ratings yet
- Philosophy of HomeopathyDocument3 pagesPhilosophy of HomeopathyRakesh ShindheNo ratings yet
- Homoeopathy in A Case of Palmo-Plantar Psoriasis: A Case ReportDocument5 pagesHomoeopathy in A Case of Palmo-Plantar Psoriasis: A Case ReportHomoeopathic PulseNo ratings yet
- Role, Prospects, and Limitation of HomoeopathyDocument43 pagesRole, Prospects, and Limitation of HomoeopathyDr.bhagyaNo ratings yet
- Homoeopathic PharmacyDocument35 pagesHomoeopathic PharmacyPranav PawarNo ratings yet
- A Case of Lateral Rectus Palsy by DR Sunil KannadaDocument5 pagesA Case of Lateral Rectus Palsy by DR Sunil KannadaHomoeopathic Pulse100% (1)
- China 200 Uses, Benefits - Cinchona Officinalis 30Document7 pagesChina 200 Uses, Benefits - Cinchona Officinalis 30subratNo ratings yet
- Free As A Bird by Markus Kuntosch Reading ExtractDocument23 pagesFree As A Bird by Markus Kuntosch Reading ExtractTariq Mehmood0% (1)
- Community Health One LinersDocument30 pagesCommunity Health One LinersRatan YadavNo ratings yet
- A Homeopathic Approach To Acute PharyngitisDocument7 pagesA Homeopathic Approach To Acute PharyngitisNadeem KhanNo ratings yet
- My Thesis Mm2Document179 pagesMy Thesis Mm2Karthik SelvamNo ratings yet
- A Thesis On Homoeopathic Management of GoutDocument3 pagesA Thesis On Homoeopathic Management of GouthirenNo ratings yet
- DISSERTATIonDocument101 pagesDISSERTATIonSukhada NimbhorkarNo ratings yet
- Fire FlyDocument10 pagesFire FlyMuralidaran SelvarajNo ratings yet
- Immunoglobulins and Homoeopathy: © Dr. Rajneesh Kumar Sharma MD (Homoeopathy) Dr. (KM) Ruchi Rajput BHMSDocument6 pagesImmunoglobulins and Homoeopathy: © Dr. Rajneesh Kumar Sharma MD (Homoeopathy) Dr. (KM) Ruchi Rajput BHMSDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Criteria For The Selection of Rubrics in A Chronic CaseDocument19 pagesCriteria For The Selection of Rubrics in A Chronic CaseVirag PatilNo ratings yet
- Comparison Repertory PDFDocument3 pagesComparison Repertory PDFDr Nimit ShahNo ratings yet
- Parenteral MedicationDocument36 pagesParenteral Medicationupendrabpkihs100% (2)
- My Experience in A Case of Haemorrhoids: Prescribing On Alternating Symptoms by DR Shelly AroraDocument5 pagesMy Experience in A Case of Haemorrhoids: Prescribing On Alternating Symptoms by DR Shelly AroraHomoeopathic Pulse100% (1)
- Bhms HomoeopathyDocument74 pagesBhms Homoeopathyprince19000% (1)
- A CASE of Acne VulgarisDocument4 pagesA CASE of Acne VulgarisHomoeopathic Pulse100% (1)
- EndometriosisDocument4 pagesEndometriosislokesh_arya1No ratings yet
- Susceptibility, Reaction, Immunity - Stuart CloseDocument57 pagesSusceptibility, Reaction, Immunity - Stuart CloseForam Patel100% (2)
- A Case of Molluscum ContagiosumDocument5 pagesA Case of Molluscum ContagiosumHomoeopathic PulseNo ratings yet
- Articles of FISHER, A. L.Document4 pagesArticles of FISHER, A. L.Muhammad Ata Ul MustafaNo ratings yet
- Computer RepertoryDocument13 pagesComputer RepertoryNikhilesha SheteNo ratings yet
- Pulse Polio Immunization IndiaDocument31 pagesPulse Polio Immunization IndiaBhumika RathoreNo ratings yet
- Laboratory FindingsDocument107 pagesLaboratory FindingsTanvir IslamNo ratings yet
- Naloxone in AdultsDocument8 pagesNaloxone in AdultsRoboschi StefaniaNo ratings yet
- Anti Protozoal AgentsDocument19 pagesAnti Protozoal AgentsNithish SNo ratings yet
- Scope and Limitation of HomoeopathyDocument10 pagesScope and Limitation of HomoeopathyPrathmesh kambleNo ratings yet
- Acute and Chronic InflammationDocument71 pagesAcute and Chronic InflammationTheBoss 20No ratings yet
- Intertrigo and Secondary Skin InfectionsDocument5 pagesIntertrigo and Secondary Skin Infectionskhalizamaulina100% (1)
- CCRH IMR Repeort PDFDocument23 pagesCCRH IMR Repeort PDFRajesh RajendranNo ratings yet
- Experience With Homoeopathy in A Case of Fibroadenoma of BreastDocument8 pagesExperience With Homoeopathy in A Case of Fibroadenoma of BreastHomoeopathic PulseNo ratings yet
- Solid Waste Management For Hospitals: Presented By: Faisal V A MT15CTM004Document46 pagesSolid Waste Management For Hospitals: Presented By: Faisal V A MT15CTM004vnitceNo ratings yet
- History of Homoeopathy in IndiaDocument44 pagesHistory of Homoeopathy in Indiaamit100% (1)
- Unit 1 - Health Psychology - FinalDocument27 pagesUnit 1 - Health Psychology - FinalSafa Maryam Khan100% (1)
- R.T. Cooper PDFDocument5 pagesR.T. Cooper PDFmihaipopescu0No ratings yet
- BTBP Repertory DR Dhwanika DhagatDocument39 pagesBTBP Repertory DR Dhwanika DhagatDrx Rustom AliNo ratings yet
- Micro paraDocument7 pagesMicro paraAj MillanNo ratings yet
- Rawat - Materia Medica of 33 Useful RemediesDocument25 pagesRawat - Materia Medica of 33 Useful RemediesMahmood MuftiNo ratings yet
- Physical Method of Microbial ControlDocument30 pagesPhysical Method of Microbial ControlAyu WidyaNo ratings yet
- Simple SubstanceDocument13 pagesSimple SubstanceHetvi ParmarNo ratings yet
- K - 1 Perspective and The Future of OncologyDocument36 pagesK - 1 Perspective and The Future of OncologyNurul Bahirah RamlyNo ratings yet
- Homoeopathic Drug Pictures Margaret Lucy Tyler.10786 3lycopodiumDocument12 pagesHomoeopathic Drug Pictures Margaret Lucy Tyler.10786 3lycopodiumhaseebwebNo ratings yet
- A Clinical Experience Natrum Mur Cures A Female With MenorrhagiaDocument4 pagesA Clinical Experience Natrum Mur Cures A Female With MenorrhagiaHomoeopathic PulseNo ratings yet
- Jugal Kishore's CardrepertoryDocument26 pagesJugal Kishore's Cardrepertorydipgang7174No ratings yet
- ENDOMETRIOSISsDocument27 pagesENDOMETRIOSISsNouman HameedNo ratings yet
- Homeopathy For HorsesDocument1 pageHomeopathy For HorsesClaire AllsopNo ratings yet
- Neurogenic FeverDocument6 pagesNeurogenic FeverTomas GuzmanNo ratings yet
- Guideline For Gout ManagementDocument28 pagesGuideline For Gout ManagementbestmonkeyNo ratings yet
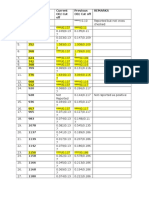
- Seria L No. Lab Number Current OD/ Cut of Previous OD/ Cut of RemarksDocument3 pagesSeria L No. Lab Number Current OD/ Cut of Previous OD/ Cut of RemarksQazi Muhammad IqbalNo ratings yet
- Annual Requirement 2016Document8 pagesAnnual Requirement 2016Qazi Muhammad IqbalNo ratings yet
- Hajj English Letter Size PDFDocument2 pagesHajj English Letter Size PDFQazi Muhammad IqbalNo ratings yet
- Arabic in 10minutes A Day PDFDocument134 pagesArabic in 10minutes A Day PDFHassan Funsho AkandeNo ratings yet
- 2015 AHA Guidelines Highlights EnglishDocument36 pages2015 AHA Guidelines Highlights EnglishshiloinNo ratings yet
- Dr. Qazi Mohammad Iqbal Community MedicineDocument2 pagesDr. Qazi Mohammad Iqbal Community MedicineQazi Muhammad IqbalNo ratings yet
- 002 Surah Al-BaqarahDocument155 pages002 Surah Al-BaqarahQazi Muhammad IqbalNo ratings yet
- Knowledge, Attitude and Practice (Kap) Study OnDocument52 pagesKnowledge, Attitude and Practice (Kap) Study OnQazi Muhammad IqbalNo ratings yet
- Mortality ReportDocument17 pagesMortality ReportQazi Muhammad IqbalNo ratings yet
- Antibiotics Lloyd ADocument11 pagesAntibiotics Lloyd AAndrew Lloyd100% (1)
- SSC CGL Tier-2 English Challenge 30 Questions - Free PDF: WWW - Careerpower.inDocument7 pagesSSC CGL Tier-2 English Challenge 30 Questions - Free PDF: WWW - Careerpower.inIshika SankhariNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- 9th-10-11th May-2016 Papers (1650 MCQS) by Amlodipine Besylate PDFDocument161 pages9th-10-11th May-2016 Papers (1650 MCQS) by Amlodipine Besylate PDFAmlodipine BesylateNo ratings yet
- History of Penicillin: Jump To Navigation Jump To SearchDocument5 pagesHistory of Penicillin: Jump To Navigation Jump To SearchRonaldNo ratings yet
- Diagnostic Testing For Sars-Cov-2: Interim Guidance 11 September 2020Document20 pagesDiagnostic Testing For Sars-Cov-2: Interim Guidance 11 September 2020Huy Trần ThiệnNo ratings yet
- Brucellosis 2Document40 pagesBrucellosis 2xcalibursysNo ratings yet
- BCC, Laboratory Specimens and Microscopy, MLT 1040, FINAL EXAM GRADEDocument24 pagesBCC, Laboratory Specimens and Microscopy, MLT 1040, FINAL EXAM GRADEalphacetaNo ratings yet
- What Is Neisseria GonorrhoeaeDocument8 pagesWhat Is Neisseria GonorrhoeaeRosNo ratings yet
- Journal IPSG 5Document7 pagesJournal IPSG 5marissa ulkhairNo ratings yet
- HIV Counselling and Testing: Dr. Kanupriya Chturvedi Dr. S.K.ChaturvediDocument22 pagesHIV Counselling and Testing: Dr. Kanupriya Chturvedi Dr. S.K.ChaturvediNasrul WahdiNo ratings yet
- Observational Study of Safe Injection Practices in A Tertiary Care Teaching HospitalDocument5 pagesObservational Study of Safe Injection Practices in A Tertiary Care Teaching HospitalMuhammad HaezarNo ratings yet
- Moraxela CatarhalisDocument20 pagesMoraxela Catarhalisshinwar benyamenNo ratings yet
- Dentalpharmacology1 130726101143 Phpapp02Document44 pagesDentalpharmacology1 130726101143 Phpapp02Malatesh Sudharshan100% (1)
- Gastroenteritis and ColitisDocument47 pagesGastroenteritis and ColitishaikalhjNo ratings yet
- Care For Elderly - TAGALOGDocument29 pagesCare For Elderly - TAGALOGKarl Kevin MarbellaNo ratings yet
- NID Report January 2013 Day 1 - 2 - 3Document10 pagesNID Report January 2013 Day 1 - 2 - 3Prabir Kumar ChatterjeeNo ratings yet
- Crab EggsDocument7 pagesCrab EggsNinfa LansangNo ratings yet
- Avian Immune System - 1Document12 pagesAvian Immune System - 1Amer AdasNo ratings yet
- Xxiii Silae Abstracts BookDocument456 pagesXxiii Silae Abstracts BookAbdo SuNo ratings yet
- PrezentareBI PMDocument51 pagesPrezentareBI PMPlic MihaelaNo ratings yet
- Implementation of The Filmarray Me Panel in Laboratory Routine Using A Simple Sample Selection Strategy For Diagnosis of Meningitis and EncephalitisDocument9 pagesImplementation of The Filmarray Me Panel in Laboratory Routine Using A Simple Sample Selection Strategy For Diagnosis of Meningitis and EncephalitisMohinish SNo ratings yet
- (MICRO2) Gram Negative CocciDocument41 pages(MICRO2) Gram Negative CocciMadhu MithaNo ratings yet
- Sterilization and DisinfectionDocument78 pagesSterilization and DisinfectionMuhammad Shoaib50% (2)
- Approach To SplenomegalyDocument37 pagesApproach To SplenomegalySarath Menon R100% (1)
- NCP Samin BabyDocument2 pagesNCP Samin BabyVioleta SomeraNo ratings yet
- CrisisplanDocument7 pagesCrisisplanapi-299225402No ratings yet
- Nelson JaundiceDocument7 pagesNelson JaundiceJesly CharliesNo ratings yet
- Patogenesis Hiv Aids PDFDocument25 pagesPatogenesis Hiv Aids PDFAyu RahmaNo ratings yet
- Liver CancerDocument233 pagesLiver CancerandikhgNo ratings yet