You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- TOEFL TEST Dan Kunci JawabanDocument5 pagesTOEFL TEST Dan Kunci JawabanwirdahajaNo ratings yet
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic FeverwirdahajaNo ratings yet
- DIG Trauma HeparDocument37 pagesDIG Trauma HeparwirdahajaNo ratings yet
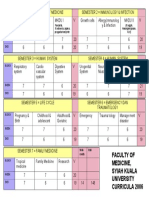
- Faculty of Medicine, Syiah Kuala University Curricula 2006Document1 pageFaculty of Medicine, Syiah Kuala University Curricula 2006wirdahajaNo ratings yet
- Tinea UnguiumDocument8 pagesTinea UnguiumwirdahajaNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- Atopic DermatitisDocument19 pagesAtopic DermatitiswirdahajaNo ratings yet
- Microbiology - Scabies and PediculosisDocument32 pagesMicrobiology - Scabies and PediculosiswirdahajaNo ratings yet
- Diagnosis BandingDocument7 pagesDiagnosis BandingHari PranotoNo ratings yet
- Diagnosis BandingDocument7 pagesDiagnosis BandingHari PranotoNo ratings yet
- IRIS Retina ExplanationsDocument19 pagesIRIS Retina ExplanationsBalraj GangadharNo ratings yet
- Follow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiDocument4 pagesFollow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiwirdahajaNo ratings yet
- Anatomy of The Ear HearingDocument14 pagesAnatomy of The Ear HearingwirdahajaNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- Fever and RashDocument14 pagesFever and RashwirdahajaNo ratings yet
- ABSES HATI-SytDocument29 pagesABSES HATI-SytwirdahajaNo ratings yet
- Abdominal PainDocument38 pagesAbdominal PainSusi Muharni RismaNo ratings yet
- Defense Mechanism (IB)Document60 pagesDefense Mechanism (IB)wirdahajaNo ratings yet
- Clinical PathwayDocument154 pagesClinical Pathwaywirdahaja100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Matarese2012 PDFDocument11 pagesMatarese2012 PDFYacine Tarik AizelNo ratings yet
- Bruno, Gene - Using Betaine Hydrochloride & Digestive Enzymes For Indigestion - Huntington College (2014)Document3 pagesBruno, Gene - Using Betaine Hydrochloride & Digestive Enzymes For Indigestion - Huntington College (2014)pedpixNo ratings yet
- IntussusceptionDocument19 pagesIntussusceptionarialNo ratings yet
- GastritisDocument37 pagesGastritisNurul Hidayah R100% (1)
- Intestinal MetaplasiaDocument12 pagesIntestinal MetaplasiaarifNo ratings yet
- Lab Report, Fargana IslamDocument5 pagesLab Report, Fargana IslamMD Fahad MiajiNo ratings yet
- Diarrhea Cmap ScriptDocument5 pagesDiarrhea Cmap ScriptmaryNo ratings yet
- l8 Management of Perianal Pain and ConditionsDocument51 pagesl8 Management of Perianal Pain and ConditionsMohd Johari Mohd ShafuwanNo ratings yet
- Bowel Obstruction - ppt1Document30 pagesBowel Obstruction - ppt1Elfrida Aulia100% (1)
- DIAARRHEADocument23 pagesDIAARRHEARudri Pandya Shukla100% (1)
- ERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineDocument24 pagesERCP-related Adverse Events: European Society of Gastrointestinal Endoscopy (ESGE) GuidelineFarid RakhmanNo ratings yet
- An Approach To Small Bowel ObstructionDocument3 pagesAn Approach To Small Bowel ObstructionHardik JeenaNo ratings yet
- 5 Pancreatita Cronica - 2011 - Eng 1Document85 pages5 Pancreatita Cronica - 2011 - Eng 1lungu eduardNo ratings yet
- Bile Peritonitis 2021Document6 pagesBile Peritonitis 2021Brvo CruzNo ratings yet
- Gall Stone CleanseDocument11 pagesGall Stone CleanseLoyiso GumaNo ratings yet
- 1.study of Physiological Functions of Digestive System of Farm AnimalsDocument58 pages1.study of Physiological Functions of Digestive System of Farm AnimalsKashifNo ratings yet
- 2015 Book TheImpactOfFoodBioactivesOnHea PDFDocument341 pages2015 Book TheImpactOfFoodBioactivesOnHea PDFVALERIA TORRES VIÑUELANo ratings yet
- COLONOSCOPY - Details: Study ResultDocument5 pagesCOLONOSCOPY - Details: Study ResultJaskaran SinghNo ratings yet
- Ulcirex CapsuleDocument3 pagesUlcirex Capsulehk_scribdNo ratings yet
- Student Guide To The Frog Dissection PDFDocument3 pagesStudent Guide To The Frog Dissection PDFSheena SemineNo ratings yet
- Requirement IPM 2019Document36 pagesRequirement IPM 2019reny noviawatiNo ratings yet
- Life Processes (Nutrition)Document4 pagesLife Processes (Nutrition)Rajender Kumar SharmaNo ratings yet
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- Bahasa Inggris Speech Class Program DiarrheaDocument4 pagesBahasa Inggris Speech Class Program Diarrheadiana ratriNo ratings yet
- LIVER PROFILE LFT Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageLIVER PROFILE LFT Test Report Format Example Sample Template Drlogy Lab ReportM ShafiqNo ratings yet
- Liver Function and AnatomyDocument2 pagesLiver Function and AnatomyKeanna Nicole CollantesNo ratings yet
- Dygestive SystemDocument21 pagesDygestive Systemapi-3731257No ratings yet
- Pyloric StenosisDocument5 pagesPyloric StenosisfdgrgNo ratings yet
- Adult Rectal Prolapse and Altemeiers Rectosigmoidectomy Current Status and The Place of Perineal RepairsDocument11 pagesAdult Rectal Prolapse and Altemeiers Rectosigmoidectomy Current Status and The Place of Perineal RepairsWorld Journal of Clinical SurgeryNo ratings yet
- Digestive Hormones and EnzymesDocument2 pagesDigestive Hormones and EnzymesTiannaNo ratings yet