You might also like
- Case Study Analysis - WeWorkDocument8 pagesCase Study Analysis - WeWorkHervé Kubwimana50% (2)
- Teacher'S Individual Plan For Professional Development SCHOOL YEAR 2020-2021Document2 pagesTeacher'S Individual Plan For Professional Development SCHOOL YEAR 2020-2021Diether Mercado Padua100% (8)
- Differential Calculus ExamDocument6 pagesDifferential Calculus ExamCaro Kan LopezNo ratings yet
- MalariaDocument41 pagesMalariaMohiuddin AhmedNo ratings yet
- Dr. Rai Muhammad Asghar Associate Professor Pediatrics Head of Pediatric Department RMC RawalpindiDocument34 pagesDr. Rai Muhammad Asghar Associate Professor Pediatrics Head of Pediatric Department RMC RawalpindiHassan AhmadNo ratings yet
- Complicated MalariaDocument56 pagesComplicated MalariaAmina MgunyaNo ratings yet
- Anemia in PregnancyDocument110 pagesAnemia in PregnancyMonika shankarNo ratings yet
- Alyana Ellaine S. Matias, MDDocument24 pagesAlyana Ellaine S. Matias, MDAlyana MatiasNo ratings yet
- Nephro Meets OncoDocument90 pagesNephro Meets OncoRenal Association MauritiusNo ratings yet
- HematuriaDocument42 pagesHematuriaAhmad SobihNo ratings yet
- Anaesthetic Implications in Concurrent DiseasesDocument37 pagesAnaesthetic Implications in Concurrent DiseasesJeevan KumarNo ratings yet
- Parasitic Infection HematologyDocument13 pagesParasitic Infection Hematologyandebetgetnet78No ratings yet
- Internal Medicine Long Case 5Document7 pagesInternal Medicine Long Case 5RoshilNo ratings yet
- Common Renal DiseasesDocument59 pagesCommon Renal DiseasesBegashawNo ratings yet
- Passmedicine MRCP Notes-NephrologyDocument73 pagesPassmedicine MRCP Notes-Nephrologysalwabeshir542No ratings yet
- Anaemia: by Swaathi R Final Year MbbsDocument33 pagesAnaemia: by Swaathi R Final Year MbbsGopi NathNo ratings yet
- Malaria: Muhammad Ulul Amrie, S.kepDocument39 pagesMalaria: Muhammad Ulul Amrie, S.kepAmrie IamNo ratings yet
- 8bone Marrow FailureDocument30 pages8bone Marrow FailureanonacadsNo ratings yet
- Acute Renal FailureDocument47 pagesAcute Renal FailureBarryKuppNo ratings yet
- 74 Acute Renal Failure UpdatedDocument48 pages74 Acute Renal Failure UpdatedaweleNo ratings yet
- Hematuria in ChildrenDocument27 pagesHematuria in ChildrenKousik AmancharlaNo ratings yet
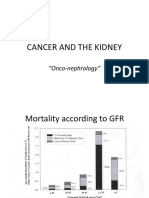
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]No ratings yet
- Malaria UnderstandingDocument29 pagesMalaria UnderstandingAmit yadavNo ratings yet
- Pancytopenia: Clinical Approach: Ajai Kumar Garg, AK Agarwal, GD SharmaDocument5 pagesPancytopenia: Clinical Approach: Ajai Kumar Garg, AK Agarwal, GD SharmaYudhistiraNo ratings yet
- Acute Promyelocytic LeukemiaDocument16 pagesAcute Promyelocytic LeukemiaMoataz TrabehNo ratings yet
- Nephrotic Syndrome in Adult (Bahan Kuliah)Document49 pagesNephrotic Syndrome in Adult (Bahan Kuliah)Jkp PhieNo ratings yet
- Puntos Clave: CAPÍTULO 108: Pancreatitis AgudaDocument15 pagesPuntos Clave: CAPÍTULO 108: Pancreatitis Agudamelani quispeNo ratings yet
- Glomerular Diseases: DR Rashmi NazarethDocument49 pagesGlomerular Diseases: DR Rashmi NazarethRohit RajeevanNo ratings yet
- Hemolytic AnemiaDocument99 pagesHemolytic AnemiaSagar Chandrakant Mhetre100% (3)
- Malaria 1Document28 pagesMalaria 1Ivy KapendaNo ratings yet
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDocument42 pagesChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulNo ratings yet
- Hematological Disorders Hematological Disorders: Renzn405Document23 pagesHematological Disorders Hematological Disorders: Renzn405Jhodie PabalanNo ratings yet
- G 6 PDDocument45 pagesG 6 PDPat TuazonNo ratings yet
- Causes of Acute Renal FailureDocument11 pagesCauses of Acute Renal FailureAndrea Roman chavezNo ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- 10.27.06 Cox Aplastic AnemiaDocument15 pages10.27.06 Cox Aplastic Anemiaravi2kanthNo ratings yet
- Clinical Aspect of MalariaDocument68 pagesClinical Aspect of MalariaselviaNo ratings yet
- Acute Renal Failure or Acute Kidney InjuryDocument8 pagesAcute Renal Failure or Acute Kidney InjuryHemanth PrakashNo ratings yet
- GlomerulonephritisDocument59 pagesGlomerulonephritistressNo ratings yet
- Microsoft PowerPoint - KNUST-LECT-STUDENT MALARIA (Compatibility Mode)Document9 pagesMicrosoft PowerPoint - KNUST-LECT-STUDENT MALARIA (Compatibility Mode)AnastasiafynnNo ratings yet
- PABROADocument5 pagesPABROAlai cruzNo ratings yet
- An Approach To Bleeding DisordersDocument30 pagesAn Approach To Bleeding DisordersSiddique BhattiNo ratings yet
- PlasmapheresisDocument2 pagesPlasmapheresispathoTMNo ratings yet
- Approach To AnemiaDocument33 pagesApproach To AnemiaVaibhav KrishnaNo ratings yet
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoNo ratings yet
- Lec 2Document10 pagesLec 2fbbqbcht6yNo ratings yet
- Malaria: Dr. Shree Narayan Yadav Internal Medicine Resident NamsDocument40 pagesMalaria: Dr. Shree Narayan Yadav Internal Medicine Resident Namsasyanadhikary18No ratings yet
- Approach To Aniemia in ChildrenDocument33 pagesApproach To Aniemia in Childrenvidya RamisettiNo ratings yet
- Disorders of Red Blood CellsDocument27 pagesDisorders of Red Blood Cellskirti sharmaNo ratings yet
- Approach To Hematuria: DR - Rinsha Ravi Dept - of Pediatrics Sath TVMDocument40 pagesApproach To Hematuria: DR - Rinsha Ravi Dept - of Pediatrics Sath TVMAnoop ThoombayilNo ratings yet
- Renal Transplantation An OverviewDocument58 pagesRenal Transplantation An OverviewSony's TechNo ratings yet
- Malaria HODocument45 pagesMalaria HOnitsuhNo ratings yet
- Liver Cirrhosis and Its ComplicationsDocument34 pagesLiver Cirrhosis and Its ComplicationsEthel ChakotaNo ratings yet
- Management of Complicated MalariaDocument36 pagesManagement of Complicated MalariaAnu SinhaNo ratings yet
- Disseminated Intravascular CoagulationDocument29 pagesDisseminated Intravascular CoagulationAnju RadhikaNo ratings yet
- Normal ValuesDocument3 pagesNormal ValuesNegros Occidental HousesNo ratings yet
- DOM Morning Report: Nephrotic SyndromeDocument40 pagesDOM Morning Report: Nephrotic SyndromeFizah IzanNo ratings yet
- Aplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeDocument47 pagesAplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeRahul Kumar VermaNo ratings yet
- Activity No.2 Common Laboratory ValuesDocument7 pagesActivity No.2 Common Laboratory ValuesGabriel PatalodNo ratings yet
- So Tim Penilik N10 16 Desember 2022 Finish-1Document163 pagesSo Tim Penilik N10 16 Desember 2022 Finish-1Muhammad EkiNo ratings yet
- Makerere University Is Inviting Applications For Undergraduate Admissions On Private Sponsorship For Academic Year 2015/2016Document9 pagesMakerere University Is Inviting Applications For Undergraduate Admissions On Private Sponsorship For Academic Year 2015/2016The Campus TimesNo ratings yet
- Silapathikaram 3Document37 pagesSilapathikaram 3gavinilaaNo ratings yet
- Hydropneumatic Booster Set MFDocument5 pagesHydropneumatic Booster Set MFdonchakdeNo ratings yet
- Catalogo HydronixDocument68 pagesCatalogo HydronixNANCHO77No ratings yet
- Lyka Kendall B. Adres: Personal Na ImpormasyonDocument2 pagesLyka Kendall B. Adres: Personal Na ImpormasyonKendall BarbietoNo ratings yet
- Ajsl DecisionMakingModel4RoRoDocument11 pagesAjsl DecisionMakingModel4RoRolesta putriNo ratings yet
- Malampaya Case StudyDocument15 pagesMalampaya Case StudyMark Kenneth ValerioNo ratings yet
- New Compabloc IMCP0002GDocument37 pagesNew Compabloc IMCP0002GAnie Ekpenyong0% (1)
- Geopolitica y Medio Ambiente - Tarea 4 - Evaluacion FinalDocument7 pagesGeopolitica y Medio Ambiente - Tarea 4 - Evaluacion FinalKATERINENo ratings yet
- Adigrat University: College of Engineering and Technology Department of Chemical EnginneringDocument39 pagesAdigrat University: College of Engineering and Technology Department of Chemical EnginneringSeid Aragaw100% (1)
- Mang-May-Tinh - 03a.-Dns1 - (Cuuduongthancong - Com)Document52 pagesMang-May-Tinh - 03a.-Dns1 - (Cuuduongthancong - Com)Anh Quân TrầnNo ratings yet
- Eco EssayDocument3 pagesEco EssaymanthanNo ratings yet
- BDRRM Sample Draft EoDocument5 pagesBDRRM Sample Draft EoJezreelJhizelRamosMendozaNo ratings yet
- Chemical Safety ChecklistDocument3 pagesChemical Safety ChecklistPillai Sreejith100% (10)
- Gothic ArchitectureDocument6 pagesGothic ArchitectureleeNo ratings yet
- Commercial BanksDocument11 pagesCommercial BanksSeba MohantyNo ratings yet
- Cs205-E S3dec18 KtuwebDocument2 pagesCs205-E S3dec18 KtuwebVighnesh MuralyNo ratings yet
- Space Saving, Tight AccessibilityDocument4 pagesSpace Saving, Tight AccessibilityTran HuyNo ratings yet
- Cuentos CADEDocument6 pagesCuentos CADEMäuricio E. González VegaNo ratings yet
- Abacus 1 PDFDocument13 pagesAbacus 1 PDFAli ChababNo ratings yet
- Module 4 How To Make Self-Rescue Evacuation Maps?Document85 pagesModule 4 How To Make Self-Rescue Evacuation Maps?RejieNo ratings yet
- A Project Report On "A Comparative Study Between Hero Honda Splendor+ and Its Competitors To Increase The Market Share in MUDHOL RegionDocument70 pagesA Project Report On "A Comparative Study Between Hero Honda Splendor+ and Its Competitors To Increase The Market Share in MUDHOL RegionBabasab Patil (Karrisatte)No ratings yet
- Harley Davidson U S Reportedly Uses Risk Sharing Agreements With Its Foreign SubsidiariesDocument1 pageHarley Davidson U S Reportedly Uses Risk Sharing Agreements With Its Foreign Subsidiariestrilocksp SinghNo ratings yet
- CSR Report On Tata SteelDocument72 pagesCSR Report On Tata SteelJagadish Sahu100% (1)
- Portfolio Write-UpDocument4 pagesPortfolio Write-UpJonFromingsNo ratings yet
- B2B Marketing: Chapter-8Document23 pagesB2B Marketing: Chapter-8Saurabh JainNo ratings yet