You might also like
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic FeverwirdahajaNo ratings yet
- DIG Trauma HeparDocument37 pagesDIG Trauma HeparwirdahajaNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- TOEFL TEST Dan Kunci JawabanDocument5 pagesTOEFL TEST Dan Kunci JawabanwirdahajaNo ratings yet
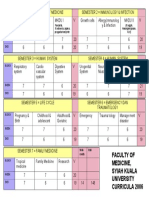
- Faculty of Medicine, Syiah Kuala University Curricula 2006Document1 pageFaculty of Medicine, Syiah Kuala University Curricula 2006wirdahajaNo ratings yet
- Diagnosis BandingDocument7 pagesDiagnosis BandingHari PranotoNo ratings yet
- Tinea UnguiumDocument8 pagesTinea UnguiumwirdahajaNo ratings yet
- Microbiology - Scabies and PediculosisDocument32 pagesMicrobiology - Scabies and PediculosiswirdahajaNo ratings yet
- Diagnosis BandingDocument7 pagesDiagnosis BandingHari PranotoNo ratings yet
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- IRIS Retina ExplanationsDocument19 pagesIRIS Retina ExplanationsBalraj GangadharNo ratings yet
- Cole StasisDocument59 pagesCole StasiswirdahajaNo ratings yet
- Anatomy of The Ear HearingDocument14 pagesAnatomy of The Ear HearingwirdahajaNo ratings yet
- Abdominal PainDocument38 pagesAbdominal PainSusi Muharni RismaNo ratings yet
- Clinical PathwayDocument154 pagesClinical Pathwaywirdahaja100% (1)
- ABSES HATI-SytDocument29 pagesABSES HATI-SytwirdahajaNo ratings yet
- Defense Mechanism (IB)Document60 pagesDefense Mechanism (IB)wirdahajaNo ratings yet
- Fever and RashDocument14 pagesFever and RashwirdahajaNo ratings yet
- Follow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiDocument4 pagesFollow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiwirdahajaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Evidence For Person-Centred Care in Chronic Wound Care: A Systematic Review and Recommendations For PracticeDocument24 pagesEvidence For Person-Centred Care in Chronic Wound Care: A Systematic Review and Recommendations For Practiceananda khairulNo ratings yet
- BCR 1976Document15 pagesBCR 1976Tia YuandaNo ratings yet
- UpToDate LecturesDocument137 pagesUpToDate Lecturesmarwa Fouad40% (5)
- Disease of SorghumDocument29 pagesDisease of SorghumVikas BhardwajNo ratings yet
- Hematological Conditions QUESTIONSDocument9 pagesHematological Conditions QUESTIONSCJ RelleveNo ratings yet
- Ibbs 2011 IndonesiaDocument80 pagesIbbs 2011 Indonesiarifka yoesoefNo ratings yet
- The Prediction of Preeclampsia The Way Forward 20Document14 pagesThe Prediction of Preeclampsia The Way Forward 20Ecaterina Sorto de ArgeñalNo ratings yet
- Oculomotor NerveDocument30 pagesOculomotor NerveBismah MudassarNo ratings yet
- Cicrulatory and Immune Workbook KEYDocument32 pagesCicrulatory and Immune Workbook KEYgeorgia robinsonNo ratings yet
- OPhtoDocument9 pagesOPhtoEkoy TheRealNo ratings yet
- Presentation On WalnutDocument5 pagesPresentation On WalnutSheikh JeelaniNo ratings yet
- 72TSO TipsSeizureObserRec 05-2019Document1 page72TSO TipsSeizureObserRec 05-2019Jasar KhanNo ratings yet
- Hydrocephalus: Signs and SymptomsDocument4 pagesHydrocephalus: Signs and SymptomsPei BartolomeNo ratings yet
- Binder Aiomt Test-8 Mock-8Document64 pagesBinder Aiomt Test-8 Mock-8naveen.jain28495No ratings yet
- Airway Pressure Release Ventilation A Review of The Evidence, Theoretical Benefits, and Alternative Titration StrategiesDocument9 pagesAirway Pressure Release Ventilation A Review of The Evidence, Theoretical Benefits, and Alternative Titration StrategiesJose Morato E FlavianeNo ratings yet
- Alexandro Bonifaz - Subcutaneous Mycoses Chromoblastomycosis, Sporotrichosis and MycetomaDocument10 pagesAlexandro Bonifaz - Subcutaneous Mycoses Chromoblastomycosis, Sporotrichosis and MycetomaElva KadarhadiNo ratings yet
- Physical Modalities For The Conservative Treatment of Wrist and Hand'sDocument28 pagesPhysical Modalities For The Conservative Treatment of Wrist and Hand'sfilipecorsairNo ratings yet
- PAPOVIRUSESDocument35 pagesPAPOVIRUSESFrancis MakanyaNo ratings yet
- Publikasi DUKUNGAN KELUARGA INGGRIS Bu IraDocument8 pagesPublikasi DUKUNGAN KELUARGA INGGRIS Bu IraRika OktarinaNo ratings yet
- Media and Information Literacy and COVID. Blog ABMdocxDocument8 pagesMedia and Information Literacy and COVID. Blog ABMdocxSherryl ZamonteNo ratings yet
- BIO MAT TESTIMONIALS - Doc0001Document30 pagesBIO MAT TESTIMONIALS - Doc0001Nicole WeatherleyNo ratings yet
- Manuscirpt IndraDocument20 pagesManuscirpt IndraIndra GunawanNo ratings yet
- Test Bank For Roachs Introductory Clinical Pharmacology 11th Edition Susan M FordDocument9 pagesTest Bank For Roachs Introductory Clinical Pharmacology 11th Edition Susan M FordLiam Perry100% (28)
- Emotion: Nature and ManagementDocument5 pagesEmotion: Nature and Managementangela alexisNo ratings yet
- Research Project - Platyhelminthes Medical Response PlanDocument26 pagesResearch Project - Platyhelminthes Medical Response PlanBammNo ratings yet
- Care of The Nose and EarDocument11 pagesCare of The Nose and EarEdmund KonoteyNo ratings yet
- Fan 2018Document4 pagesFan 2018Илија РадосављевићNo ratings yet
- Quarter 3: Module 4 (Weeks 4-5) Nature of Emerging and Re-Emerging DiseasesDocument19 pagesQuarter 3: Module 4 (Weeks 4-5) Nature of Emerging and Re-Emerging DiseasesGeceylNo ratings yet
- Circadian ClockspdfDocument5 pagesCircadian ClockspdfGuimacNo ratings yet
- MATERIAL SAFETY DATA SHEET - FrickDocument13 pagesMATERIAL SAFETY DATA SHEET - FricksanNo ratings yet