You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Bantuan Hidup Dasar Dan Lanjut: BHD-BHLDocument38 pagesBantuan Hidup Dasar Dan Lanjut: BHD-BHLIda Benecia DeseNo ratings yet
- Daily Report: Tanggal/Jam Ruangan KegiatanDocument2 pagesDaily Report: Tanggal/Jam Ruangan KegiatanIda Benecia DeseNo ratings yet
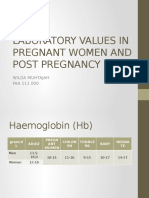
- Laboratory Values in Pregnant Women and Post PregnancyDocument7 pagesLaboratory Values in Pregnant Women and Post PregnancyIda Benecia DeseNo ratings yet
- Tanda Vital Jenis Cairan Obat - Obatan Pemasangan Alat KeteranganDocument1 pageTanda Vital Jenis Cairan Obat - Obatan Pemasangan Alat KeteranganIda Benecia DeseNo ratings yet
- Soft Tissue Uvea Disease JournalDocument65 pagesSoft Tissue Uvea Disease JournalIda Benecia DeseNo ratings yet
- Soft Tissue Uvea Disease JournalDocument65 pagesSoft Tissue Uvea Disease JournalIda Benecia DeseNo ratings yet
- Increased of Intracranial Pressure and Brain Herniation SyndromeDocument33 pagesIncreased of Intracranial Pressure and Brain Herniation SyndromeIda Benecia DeseNo ratings yet
- AterosklerosisDocument40 pagesAterosklerosisIda Benecia DeseNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Musculoskeletal PhysiologyDocument5 pagesMusculoskeletal PhysiologyKhairul IkhwanNo ratings yet
- Anti-Cholinergic Drugs and Cholinesterase InhibitorsDocument24 pagesAnti-Cholinergic Drugs and Cholinesterase InhibitorsKhalid I. Abdullah100% (1)
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- 610R0110A5 ForbiddenCuresUndrgrndMed WebDocument175 pages610R0110A5 ForbiddenCuresUndrgrndMed Webshakti-babalon100% (10)
- Physiology Notes Semester 1Document84 pagesPhysiology Notes Semester 1Daniel Li100% (1)
- Neuronal CommunicationDocument9 pagesNeuronal CommunicationNatalia RamirezNo ratings yet
- Organophosphate Poisoning - WikiDocument31 pagesOrganophosphate Poisoning - WikiLIDIYA MOL P VNo ratings yet
- Neuromuscular Physiology ExperimentDocument18 pagesNeuromuscular Physiology ExperimentmenschNo ratings yet
- Neurotransmitters &: Their Mode of ActionDocument45 pagesNeurotransmitters &: Their Mode of ActionAshani AaroraNo ratings yet
- Pharmacology and Allied Subjects by Hema Seliya Jul 02 2022 06-34-09 20 PM 3Document20 pagesPharmacology and Allied Subjects by Hema Seliya Jul 02 2022 06-34-09 20 PM 3Huba ZehraNo ratings yet
- NCM 106 Module 5FDocument22 pagesNCM 106 Module 5FMega SoundNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyDocument3 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: PhysiologyMavic Villanueva100% (1)
- Old Is GoldDocument144 pagesOld Is Goldnreena aslamNo ratings yet
- Biological Approach Booklet 2021Document41 pagesBiological Approach Booklet 2021Abigail HARTNo ratings yet
- Pharmacology Viva QuestionsDocument24 pagesPharmacology Viva QuestionsMinhaz Islam100% (1)
- Nerve Muscle PhysioDocument30 pagesNerve Muscle Physiopatel_hanisha06No ratings yet
- (Cholinergic System) Model Questions and AnswersDocument45 pages(Cholinergic System) Model Questions and AnswersAjay SinghNo ratings yet
- PHC 513 Flipped Class QuestionDocument17 pagesPHC 513 Flipped Class QuestionALISYA SOPHIA MOHAMMAD ABU SHAHID CHRISNo ratings yet
- Neuromuscular Blocking AgentsDocument18 pagesNeuromuscular Blocking AgentsLalibah AntartikaNo ratings yet
- Antiparasitc PharmacologyDocument153 pagesAntiparasitc PharmacologyMohanad Al-BayatiNo ratings yet
- (Oklahoma Notes) Roger Thies Ph.D. (Auth.), Roger Thies Ph.D. (Eds.) - Physiology-Springer-Verlag New York (1995)Document287 pages(Oklahoma Notes) Roger Thies Ph.D. (Auth.), Roger Thies Ph.D. (Eds.) - Physiology-Springer-Verlag New York (1995)MaadaNo ratings yet
- EnvironmentDocument9 pagesEnvironmentrimantasjankusNo ratings yet
- Non-Depolarising Blockers Depolarising Blockers Botox: Anticholinesterase IMPORTANTDocument2 pagesNon-Depolarising Blockers Depolarising Blockers Botox: Anticholinesterase IMPORTANTjsdlzjNo ratings yet
- Medical-Surgical Nursing ReviewDocument90 pagesMedical-Surgical Nursing Reviewɹǝʍdןnos99% (312)
- Chapter 2. WCUDocument75 pagesChapter 2. WCUethiomoney15No ratings yet
- Psychology A Concise Introduction 5th Edition Griggs Test BankDocument52 pagesPsychology A Concise Introduction 5th Edition Griggs Test BankPat Ochs100% (40)
- Yu-Chen Lee PHYS20100 - ContinuousAssessment - Assignment#3 - WorksheetDocument5 pagesYu-Chen Lee PHYS20100 - ContinuousAssessment - Assignment#3 - Worksheet李雨宸No ratings yet
- Diacylglycerol Lipase A ManipulationDocument9 pagesDiacylglycerol Lipase A ManipulationKis AlexandraNo ratings yet
- Case Studies On Major Concepts: NeurologicalDocument37 pagesCase Studies On Major Concepts: NeurologicalJek Dela CruzNo ratings yet
- Long-Term Effects of Repeated Botulinum Toxin Injection in Cosmetic Therapeutics - Crook, 2022Document8 pagesLong-Term Effects of Repeated Botulinum Toxin Injection in Cosmetic Therapeutics - Crook, 2022Rafael Autran Cavalcante AraújoNo ratings yet