You might also like
- Synthesis: Repertorium Homoeopathicum SyntheticumDocument29 pagesSynthesis: Repertorium Homoeopathicum SyntheticumSk Saklin Mustak67% (3)
- Acute Respiratory FailureDocument29 pagesAcute Respiratory FailurePurnima ChoudhuryNo ratings yet
- MAPEH 9 TOS 1st GradingDocument4 pagesMAPEH 9 TOS 1st Gradingelyn50% (2)
- Nutrition Notes in TableDocument31 pagesNutrition Notes in TableJan Oliver YaresNo ratings yet
- Alterations in Gas Exchange NEW SU 2023 STUDENTDocument83 pagesAlterations in Gas Exchange NEW SU 2023 STUDENTHaley HannNo ratings yet
- Dr. K. V. Raman, Dean, MtpgrihsDocument66 pagesDr. K. V. Raman, Dean, MtpgrihsShruti100% (1)
- Pneumonia (Pulmonya)Document33 pagesPneumonia (Pulmonya)LopaoMedinaNo ratings yet
- Di, Siadh, CSW Tabel PerbedaanDocument17 pagesDi, Siadh, CSW Tabel PerbedaanMichael Tambunan100% (1)
- Icpc 2 R PDFDocument204 pagesIcpc 2 R PDFagni sukma fahiraNo ratings yet
- CHF NanananananananannaDocument19 pagesCHF NanananananananannaKhairatul Laila INo ratings yet
- Planned Teaching On Occupational Health HazardsDocument8 pagesPlanned Teaching On Occupational Health HazardsgandhialpitNo ratings yet
- LP PneumoniaDocument12 pagesLP PneumoniaFebri AstutiNo ratings yet
- Jurnal Pengaruh Kukusan Labu Terhadap Tekanan DarahDocument13 pagesJurnal Pengaruh Kukusan Labu Terhadap Tekanan DarahAyudiah UprianingsihNo ratings yet
- Alifa Nasyahta Rosiana 22010110110055 Bab8KTIDocument49 pagesAlifa Nasyahta Rosiana 22010110110055 Bab8KTIYudhi SetiabudiNo ratings yet
- Tugas Giving AdviceDocument9 pagesTugas Giving Adviceputri rahayuNo ratings yet
- Materi Kep. Kritis Acute GI BleedingDocument35 pagesMateri Kep. Kritis Acute GI Bleedingharsani auroraNo ratings yet
- Kandidat Skripsi Fakultas Kedokteran Universitas Sam Ratulangi Manado Bagian Ilmu Anestesi Dan Terapi Intensif Universitas Sam Ratulangi ManadoDocument8 pagesKandidat Skripsi Fakultas Kedokteran Universitas Sam Ratulangi Manado Bagian Ilmu Anestesi Dan Terapi Intensif Universitas Sam Ratulangi Manadoglorya nathasiaNo ratings yet
- Daftar Pustaka Hipertensi Pada Usia MudaDocument10 pagesDaftar Pustaka Hipertensi Pada Usia MudaToby Hadinata WiranegaraNo ratings yet
- Algoritma DkaDocument1 pageAlgoritma DkaKang KangNo ratings yet
- Diajukan Untuk Memenuhi Persyaratan Memperoleh Gelar Sarjana Keperawatan (S.Kep)Document152 pagesDiajukan Untuk Memenuhi Persyaratan Memperoleh Gelar Sarjana Keperawatan (S.Kep)ferdi ramadhaniNo ratings yet
- Acute Respiratory Distress Syndrome: Jurnal RespirasiDocument11 pagesAcute Respiratory Distress Syndrome: Jurnal RespirasiArmia UsnihidayatiNo ratings yet
- Daftar Pustaka StuntingDocument1 pageDaftar Pustaka StuntingtomoandiNo ratings yet
- Jurnal CairanDocument9 pagesJurnal Cairanapriyani ikaNo ratings yet
- Tugas Rancangan Asuhan Keperawatan Dengan Integrasi Ebp DanDocument11 pagesTugas Rancangan Asuhan Keperawatan Dengan Integrasi Ebp DanInkha LepaNo ratings yet
- Hipertiroid HarrisonDocument8 pagesHipertiroid HarrisonravenskaNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutnidaNo ratings yet
- Askep DM Tipe 1Document11 pagesAskep DM Tipe 1Tsaalits MuharrorohNo ratings yet
- Systemic Lupus Erythematosus (SLE) : Pembimbing: Dr. Sondang M Lumban Batu, Sp.ADocument36 pagesSystemic Lupus Erythematosus (SLE) : Pembimbing: Dr. Sondang M Lumban Batu, Sp.AWinda Oktavia PakpahanNo ratings yet
- Pathway PneumoniaDocument1 pagePathway PneumoniaNur Kholis ArswendoNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Gold 2019Document43 pagesGold 2019Hayatillah Natasya100% (1)
- Overview of The Mucopolysaccharidoses: RheumatologyDocument9 pagesOverview of The Mucopolysaccharidoses: RheumatologyLaura Orjuela MateusNo ratings yet
- Patoflowdiagram Fraktur (Debora Angelina Sirait)Document1 pagePatoflowdiagram Fraktur (Debora Angelina Sirait)Debora SiraitNo ratings yet
- Daftar Pustaka: / Ppok PDFDocument3 pagesDaftar Pustaka: / Ppok PDFMuhammadSyafrilNo ratings yet
- B Inggris Halim NCP Asma BronchialDocument28 pagesB Inggris Halim NCP Asma BronchialAbdul HlmNo ratings yet
- Patogenesis TBCDocument4 pagesPatogenesis TBCKiki Ayu ApsariNo ratings yet
- Jurnal HipertensiDocument5 pagesJurnal HipertensiMuhammad Ali AkbarNo ratings yet
- PDF LP Hipertensi Pada KehamilanDocument19 pagesPDF LP Hipertensi Pada KehamilanAyapuspita SariNo ratings yet
- Leaflet Cushing SyndromeDocument2 pagesLeaflet Cushing SyndromesepthyaniNo ratings yet
- Pathway Trauma DadaDocument1 pagePathway Trauma DadaAnton Pratama100% (2)
- Widya Dharma Husada: Sekolah Tinggi Ilmu KesehatanDocument4 pagesWidya Dharma Husada: Sekolah Tinggi Ilmu KesehatanWiwi Riani0% (1)
- Jurnal Acute Decompensated Heart FailureDocument4 pagesJurnal Acute Decompensated Heart FailureMayang Sri WulandNo ratings yet
- Sap Diet Rendah GaramDocument7 pagesSap Diet Rendah GaramRachmadani Ika SyafitriNo ratings yet
- Anatomi Sistem KardiovaskularDocument71 pagesAnatomi Sistem KardiovaskularGunk Iztrie Julia TensadianiNo ratings yet
- 2016-2 Data Mhs (Genap)Document132 pages2016-2 Data Mhs (Genap)dini hariyantiNo ratings yet
- Hiperkoagulasi Pada TB ParuDocument28 pagesHiperkoagulasi Pada TB Parusenoaji widodoNo ratings yet
- Anemia Hemolitik Et Causa ThalasemiaDocument47 pagesAnemia Hemolitik Et Causa ThalasemiaAnusha PrakashNo ratings yet
- Acs Tugas FixDocument52 pagesAcs Tugas FixAlsiasintaNo ratings yet
- B.inggris Laporan Pendahuluan Hipertensi-1-DikonversiDocument13 pagesB.inggris Laporan Pendahuluan Hipertensi-1-DikonversiTia AmandaNo ratings yet
- Tifoid PerforasiDocument5 pagesTifoid PerforasiSisca Dwi Agustina0% (1)
- Pathways AidsDocument1 pagePathways AidsSayhidoen CepexNo ratings yet
- Bahasa Inggris III: 13. Let's Make Nursing Report (Nursing Documentation)Document9 pagesBahasa Inggris III: 13. Let's Make Nursing Report (Nursing Documentation)Erwin PardiansyahNo ratings yet
- Satuan Acara Penyuluhan Senam Hipertensi: Disusun Oleh: Anis Nur Azizah 170104020Document10 pagesSatuan Acara Penyuluhan Senam Hipertensi: Disusun Oleh: Anis Nur Azizah 170104020Setiani CharixlaluNo ratings yet
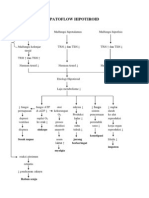
- Patoflow Hipotiroid: Sinkope Konstipasi Sesak Napas Jarang Berkeringat Impoten MyalgiaDocument1 pagePatoflow Hipotiroid: Sinkope Konstipasi Sesak Napas Jarang Berkeringat Impoten MyalgiaDessyana Paulus50% (2)
- Cardiac Arrhythmias: Abnormal of Cardiac RhythmDocument39 pagesCardiac Arrhythmias: Abnormal of Cardiac Rhythmemoyandhy100% (1)
- Askep PdaDocument44 pagesAskep Pdaririn2942No ratings yet
- Giant BullaeDocument43 pagesGiant Bullaefaishalanwar36No ratings yet
- Referensi Jurnal Jantung RematikDocument5 pagesReferensi Jurnal Jantung RematikEddogawa C' TaplakismeNo ratings yet
- 8 DAFTAR PUSTAKA Abses HeparDocument2 pages8 DAFTAR PUSTAKA Abses HeparamelNo ratings yet
- Valid BronkopneumoniaDocument37 pagesValid BronkopneumoniaKarina Diana Safitri100% (1)
- MEXA-584L E CatalogDocument2 pagesMEXA-584L E CatalogUser_docs100% (1)
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- LP AprillyaPFU 006Document28 pagesLP AprillyaPFU 006Winda ThataNo ratings yet
- Respiratory FailureDocument39 pagesRespiratory FailureMuntasir BashirNo ratings yet
- Respiratory Failure: Dr. Sat Sharma Univ of ManitobaDocument38 pagesRespiratory Failure: Dr. Sat Sharma Univ of ManitobaGonzalo Venegas RojasNo ratings yet
- Running A Race at 12,000 FeetDocument39 pagesRunning A Race at 12,000 FeetAndela Ernesto HenriqueNo ratings yet
- Tuti Herawati, MN: Fakultas Ilmu Keperawatan Universitas Indonesia 2008Document40 pagesTuti Herawati, MN: Fakultas Ilmu Keperawatan Universitas Indonesia 2008SelvyaNo ratings yet
- Paragraph DevelopmentDocument7 pagesParagraph DevelopmentJacqueline Gregorio RamosNo ratings yet
- Cuddon - Electrophysiology in Neuromuscular Disease - 2002Document32 pagesCuddon - Electrophysiology in Neuromuscular Disease - 2002paula gonzalezNo ratings yet
- This House Would Go VegetarianDocument10 pagesThis House Would Go VegetarianRatih AndariNo ratings yet
- Case Study PresentationDocument21 pagesCase Study Presentationapi-272776993No ratings yet
- Sexual HealthDocument11 pagesSexual Healthapi-236516264No ratings yet
- Word FormationDocument20 pagesWord FormationSilviu EnglishNo ratings yet
- Osteomyelitis Akut Dan KronikDocument63 pagesOsteomyelitis Akut Dan KronikAri SetiawanNo ratings yet
- Name: Kelvin Martinez Background Information:: Part 1: PBS Nova-Making VaccinesDocument3 pagesName: Kelvin Martinez Background Information:: Part 1: PBS Nova-Making VaccinesNoelNo ratings yet
- Haad QuestionDocument20 pagesHaad QuestionNimraj PatelNo ratings yet
- Talampas, Crisanto J. Psychiatry Clinical Clerk History and Mental Status ExaminationDocument4 pagesTalampas, Crisanto J. Psychiatry Clinical Clerk History and Mental Status ExaminationCrisanto TalampasNo ratings yet
- A Beautiful Mind ReviewDocument9 pagesA Beautiful Mind ReviewPatriciaChristieNo ratings yet
- The Yellow WallpaperDocument2 pagesThe Yellow Wallpaperapi-351181791No ratings yet
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaDocument106 pagesDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12No ratings yet
- Hiatal HerniaDocument6 pagesHiatal HerniaMaria Donabella OngueNo ratings yet
- Spinal Exercise Home ProgrammeDocument19 pagesSpinal Exercise Home ProgrammePrabha VetrichelvanNo ratings yet
- Jurnal Kesmas Jumal HusniDocument9 pagesJurnal Kesmas Jumal HusniHumam_Aziz_2281No ratings yet
- Miss Purkiss 135 QuestionsDocument2 pagesMiss Purkiss 135 QuestionsJemima Hui-Tung ManNo ratings yet
- Grade 5 Term 4 Life Skills Lesson Plan Name of Lesson: Become A Disease Detective!Document3 pagesGrade 5 Term 4 Life Skills Lesson Plan Name of Lesson: Become A Disease Detective!Raeesa SNo ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- Classical Western FormulasDocument4 pagesClassical Western FormulasSofia MirandaNo ratings yet
- Lecture 11cholesterol ManagementDocument19 pagesLecture 11cholesterol ManagementMahmoud Elamer ElmenshawyNo ratings yet
- Single Squamous EpitheliumDocument28 pagesSingle Squamous EpitheliumLyndonn Santos100% (1)
- AIIMS PG 2005 Question Paper PDFDocument26 pagesAIIMS PG 2005 Question Paper PDFramNo ratings yet