You might also like
- THE Anatomic and Physiologic Difference Between Child and AdultDocument15 pagesTHE Anatomic and Physiologic Difference Between Child and AdultSanthosh.S.U75% (4)
- The Philippine Human Milk BankingDocument48 pagesThe Philippine Human Milk BankingErika Cruz100% (1)
- Case Study of A Boy With HaemophiliaDocument18 pagesCase Study of A Boy With HaemophiliaImanuel Far-FarNo ratings yet
- Ileal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument5 pagesIleal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenAnonymous 7hW4aGNo ratings yet
- PoliomyelitisDocument65 pagesPoliomyelitistummalapalli venkateswara raoNo ratings yet
- PolioDocument8 pagesPolioKailash Nagar100% (1)
- Care of Unconscious ClientDocument27 pagesCare of Unconscious ClientDonelie Kay Tapel AsanzaNo ratings yet
- MumpsDocument11 pagesMumpscasandra moranteNo ratings yet
- Health Teaching of Patients With Tuberculosis TreatmentDocument34 pagesHealth Teaching of Patients With Tuberculosis TreatmentFarhanaRahimNo ratings yet
- Perineal Tear: AnatomyDocument4 pagesPerineal Tear: AnatomySuhas IngaleNo ratings yet
- CiprofloxacinDocument3 pagesCiprofloxacinapi-3797941No ratings yet
- Nursing Management of BurnDocument40 pagesNursing Management of BurnSalinKaur0% (1)
- 5 Nursing Management TBDocument2 pages5 Nursing Management TBًNo ratings yet
- Septic ArthritisDocument8 pagesSeptic ArthritisLorebell100% (2)
- OSTEOMALACIADocument6 pagesOSTEOMALACIAThine NG CalderonNo ratings yet
- Retinal DetachmentDocument7 pagesRetinal Detachmentjay dewanagnNo ratings yet
- PoliomyelitisDocument43 pagesPoliomyelitisGurpreet KaurNo ratings yet
- Tuberculosis (The Disease)Document24 pagesTuberculosis (The Disease)DiLahNo ratings yet
- PoliomyelitisDocument13 pagesPoliomyelitiscasandra morante100% (2)
- Care of HemophiliaDocument7 pagesCare of HemophiliaBasant karn100% (4)
- Dolo 650 MG (Paracetamol) : Uses, Side Effects, DosageDocument3 pagesDolo 650 MG (Paracetamol) : Uses, Side Effects, DosageRaluca Elena Raluca ElenaNo ratings yet
- Drug StudyDocument20 pagesDrug Studyvarshasharma05No ratings yet
- SplintsDocument16 pagesSplintsShini SimonNo ratings yet
- Lie PresentationDocument31 pagesLie PresentationHema Malini100% (1)
- CVA IntroductionDocument12 pagesCVA IntroductionSuzette Rae TateNo ratings yet
- BibliographyDocument2 pagesBibliographyMahesh T MadhavanNo ratings yet
- Lumbar Puncture ReportDocument5 pagesLumbar Puncture ReportTweenie DalumpinesNo ratings yet
- Malaria PreventionDocument3 pagesMalaria PreventionRohit_Patkar_2942No ratings yet
- Osteogenesis ImperfectaDocument8 pagesOsteogenesis ImperfectaDokter ZukieNo ratings yet
- Case Management of Ari at PHC LevelDocument29 pagesCase Management of Ari at PHC Levelapi-3823785No ratings yet
- Diarrhea: DefinitionDocument13 pagesDiarrhea: Definitionudaybujji100% (1)
- Congenital Talipes Equinovarus (Clubfoot)Document24 pagesCongenital Talipes Equinovarus (Clubfoot)Boetik AlifiaNo ratings yet
- A Seminar On The Topic TetanusDocument16 pagesA Seminar On The Topic TetanusRajat PadhanNo ratings yet
- ANMDocument2 pagesANMShreyas Walvekar100% (1)
- Post Term PregnancyDocument12 pagesPost Term PregnancyRizky Putra Ismeldi100% (1)
- Care of Unconscious PatientDocument5 pagesCare of Unconscious PatientRuchika Kaushal67% (3)
- What Is Rabies?Document9 pagesWhat Is Rabies?Bijay Kumar MahatoNo ratings yet
- Newborn ReflexesDocument41 pagesNewborn ReflexesUmairah Bashir100% (5)
- Tetanus Case PresentationDocument18 pagesTetanus Case PresentationDesiree Guerra100% (1)
- Anatomy and Physiology of The BreastDocument42 pagesAnatomy and Physiology of The BreastNicole SooNo ratings yet
- Pott Spine PDFDocument7 pagesPott Spine PDFdaniphilip777No ratings yet
- Femur Fracture Health EducationDocument1 pageFemur Fracture Health EducationMadx VNo ratings yet
- Myomectomy - ChandaniDocument55 pagesMyomectomy - Chandanichandani pandeyNo ratings yet
- Drug StudyDocument8 pagesDrug Studykarenkaren09No ratings yet
- Vaccines and SeraDocument19 pagesVaccines and SeraMaulik M Patel100% (1)
- Cerebral Palsy: I. Definition/ DescriptionDocument4 pagesCerebral Palsy: I. Definition/ Descriptionfaye kim100% (1)
- Hiv AidsDocument37 pagesHiv AidsAgung PriasmoyoNo ratings yet
- Wound Infection: Julie Mae T. Ambay BSN 2-2Document14 pagesWound Infection: Julie Mae T. Ambay BSN 2-2Julie Mae AmbayNo ratings yet
- PPH by Dr. Rajabu Nyangara MtillyDocument38 pagesPPH by Dr. Rajabu Nyangara MtillynyangaraNo ratings yet
- Bell - S PalsyDocument17 pagesBell - S PalsyRickzen Hawkins NikecholantNo ratings yet
- CVADocument22 pagesCVAPankaj Shahi100% (1)
- Case Study OsteoporosisDocument17 pagesCase Study Osteoporosistarikeops50% (2)
- HydrocephalusDocument25 pagesHydrocephalusعمارہ عمرNo ratings yet
- TetanusDocument28 pagesTetanusKarunya Vk100% (1)
- Difference Between Neurosis and PsychosisDocument4 pagesDifference Between Neurosis and PsychosisShaheen Khan Warsi100% (1)
- A Surgical InstrumentsDocument14 pagesA Surgical InstrumentsSanela DžanovićNo ratings yet
- Picornaviridae - CDocument9 pagesPicornaviridae - Cميمونه عبد الرحيم مصطفىNo ratings yet
- INTESTINAL INFECTIONS BhmsDocument5 pagesINTESTINAL INFECTIONS BhmsBhavithra. PNo ratings yet
- Gutierrez, Winell M. 5 NOVEMBER 2019 BSN Ii-3 Rle-Camantiles Rhu PoliomyelitisDocument6 pagesGutierrez, Winell M. 5 NOVEMBER 2019 BSN Ii-3 Rle-Camantiles Rhu PoliomyelitisWinell GutierrezNo ratings yet
- Poliomyelitis: Abarca, Mark Nerza, Lourelie BSN3-ADocument45 pagesPoliomyelitis: Abarca, Mark Nerza, Lourelie BSN3-Arhimineecat71No ratings yet
- Polio by KumkumDocument55 pagesPolio by KumkumAnkit KumarNo ratings yet
- Vaccine PreventableDocument89 pagesVaccine PreventableMohammad Doctor CabdiraxmanNo ratings yet
- Our Vison To Future On Diagnostic Microbiology by Dr.T.V.Rao MDDocument5 pagesOur Vison To Future On Diagnostic Microbiology by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- MEDICAL ETHICS IN RESEARCH PROPOSALS (Indian Contest)Document62 pagesMEDICAL ETHICS IN RESEARCH PROPOSALS (Indian Contest)tummalapalli venkateswara raoNo ratings yet
- Current Trends in Sterilisation of Operation TheatresDocument7 pagesCurrent Trends in Sterilisation of Operation Theatrestummalapalli venkateswara raoNo ratings yet
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDDocument100 pagesInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Artificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDDocument34 pagesArtificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Screening For MRSA by Dr.T.V.Rao MDDocument30 pagesScreening For MRSA by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Surgical Operation Theater StandardsDocument31 pagesSurgical Operation Theater Standardstummalapalli venkateswara raoNo ratings yet
- JOURNAL CLUB in Medicine Preparation and Presentation Dr.T.V.Rao MDDocument36 pagesJOURNAL CLUB in Medicine Preparation and Presentation Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- MDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDDocument2 pagesMDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- HOSPITAL ANTIBIOGRAMS Principles Interpretation and DocumentationDocument55 pagesHOSPITAL ANTIBIOGRAMS Principles Interpretation and Documentationtummalapalli venkateswara raoNo ratings yet
- Streaking Culture Plates in Bacteriology by Dr.T.V.Rao MDDocument33 pagesStreaking Culture Plates in Bacteriology by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Infection Control in Burns PatietnsDocument41 pagesInfection Control in Burns Patietnstummalapalli venkateswara raoNo ratings yet
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDocument2 pagesGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Who Is Killing Modern Medicine in IndiaDocument3 pagesWho Is Killing Modern Medicine in Indiatummalapalli venkateswara raoNo ratings yet
- School Hygiene by Dr.T.V.Rao MDDocument32 pagesSchool Hygiene by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Need For Clinical Microbiologists by Dr.T.V.Rao MDDocument2 pagesNeed For Clinical Microbiologists by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- Fall Out of Neet On Medical EdcuationDocument2 pagesFall Out of Neet On Medical Edcuationtummalapalli venkateswara raoNo ratings yet
- School Hygiene Preventing InfectionsDocument19 pagesSchool Hygiene Preventing Infectionstummalapalli venkateswara raoNo ratings yet
- Hand Hygiene and Prevention of Infection inDocument22 pagesHand Hygiene and Prevention of Infection intummalapalli venkateswara raoNo ratings yet
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDocument28 pagesElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- 10 Options To Control Hospital Infections by Dr.T.V.Rao MDDocument17 pages10 Options To Control Hospital Infections by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- INFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDDocument25 pagesINFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- MALDI-ToF in Clinical MicrobiologyDocument39 pagesMALDI-ToF in Clinical Microbiologytummalapalli venkateswara rao100% (1)
- MDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDDocument33 pagesMDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- INTERPRETATION OF ANTIBIOGRAMS Trends of Change by Dr.T.V.Rao MDDocument62 pagesINTERPRETATION OF ANTIBIOGRAMS Trends of Change by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDocument61 pagesHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- MDR-TB An Update by Dr.T.V.Rao MDDocument43 pagesMDR-TB An Update by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- World TB Day 2016Document33 pagesWorld TB Day 2016tummalapalli venkateswara raoNo ratings yet
- Health Care Associated Infections Creating Drug Resistance AtlasDocument46 pagesHealth Care Associated Infections Creating Drug Resistance Atlastummalapalli venkateswara raoNo ratings yet
- Simancas-Racines D, Guerra CV, Hidalgo R. Vaccines For The Common Cold (Review) .Cochrane PDFDocument3 pagesSimancas-Racines D, Guerra CV, Hidalgo R. Vaccines For The Common Cold (Review) .Cochrane PDFAlex MolinaNo ratings yet
- Classification of DiseasesDocument51 pagesClassification of Diseasesapi-446296420No ratings yet
- PD996 Compulsory ImzDocument2 pagesPD996 Compulsory Imzapi-19824701No ratings yet
- Immunization UipDocument20 pagesImmunization Uipdevesh gargNo ratings yet
- Agua de CocoDocument12 pagesAgua de Cococarlosholguinp2694No ratings yet
- VHND Field Form Cum Check List Rev 01Document3 pagesVHND Field Form Cum Check List Rev 01nishantojha0% (1)
- Documents Emerge Proving DR Andrew Wakefield Innocent BMJ and Brian Deer Caught Misrepresenting The FactsDocument5 pagesDocuments Emerge Proving DR Andrew Wakefield Innocent BMJ and Brian Deer Caught Misrepresenting The Factsjamie_clark_2100% (1)
- Reactii Adverse Vaccin Infanrix HexaDocument1,271 pagesReactii Adverse Vaccin Infanrix HexaRaluca HuzumNo ratings yet
- Expanded Program On Immunization and Reproductive Health DOH ProgramsDocument24 pagesExpanded Program On Immunization and Reproductive Health DOH ProgramsPrince Jhessie L. AbellaNo ratings yet
- HHHDocument10 pagesHHHRalu OroszNo ratings yet
- Drugs Re QuestionsDocument6 pagesDrugs Re Questionslipe167No ratings yet
- Measles Epidemic Ex - StudentDocument12 pagesMeasles Epidemic Ex - StudentMervin Ezekiel Amistoso FranciscoNo ratings yet
- Vis DtapDocument2 pagesVis DtapBeeco SiboroNo ratings yet
- MumpsDocument2 pagesMumpsArjunJainNo ratings yet
- Public Health Sector by AbhishekDocument12 pagesPublic Health Sector by AbhishekfdxgfdgbfbhNo ratings yet
- Community Health Nursing ExamDocument201 pagesCommunity Health Nursing ExamPongpong Laranjo AsuncionNo ratings yet
- Part Two ResourcesDocument4 pagesPart Two Resourcesapi-158169273No ratings yet
- Office of The Provincial Governor: Province of Oriental MindoroDocument1 pageOffice of The Provincial Governor: Province of Oriental MindoroZyreen Kate BCNo ratings yet
- Sumbad, Mark Bhen E.-Activity-6-IMCIDocument3 pagesSumbad, Mark Bhen E.-Activity-6-IMCIMb SumbadNo ratings yet
- IDSP P Forms PDFDocument2 pagesIDSP P Forms PDFNishita DughNo ratings yet
- ToshiDocument3 pagesToshihjbkhbjtNo ratings yet
- Calculo de Volúmenes en InmunizacionesDocument36 pagesCalculo de Volúmenes en InmunizacionesWalter Espinoza EspirituNo ratings yet
- Infection in PediatricDocument36 pagesInfection in PediatricSitaNo ratings yet
- TVCC Vaccination Presentation-1Document57 pagesTVCC Vaccination Presentation-1Gagandeep Singh DhamiNo ratings yet
- Center For Health Development - I: Republic of The Philippines Department of HealthDocument2 pagesCenter For Health Development - I: Republic of The Philippines Department of HealthJennifer AngNo ratings yet
- Initial Database For Family Nursing Care-HeCare1Document5 pagesInitial Database For Family Nursing Care-HeCare1tinatin989No ratings yet
- Know About Dengue FeverDocument11 pagesKnow About Dengue FeverKamlesh SanghaviNo ratings yet
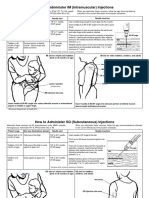
- Im SQ Admin PDFDocument2 pagesIm SQ Admin PDFAlvin JjNo ratings yet