
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Helloooukdi PDFDocument115 pagesHelloooukdi PDFIqbal HabibieNo ratings yet
- IT 1 - Funduscopic Examination (2) - RZDocument15 pagesIT 1 - Funduscopic Examination (2) - RZIqbal HabibieNo ratings yet
- Preterm Labor1Document61 pagesPreterm Labor1Somaira HassanNo ratings yet
- Iqbal Lisa-HDL Post Ator LitorDocument2 pagesIqbal Lisa-HDL Post Ator LitorIqbal HabibieNo ratings yet
- Primary Care of Musculoskeletal Problems in The Outpatient SDocument350 pagesPrimary Care of Musculoskeletal Problems in The Outpatient SIqbal HabibieNo ratings yet
- IT 5 - Visual Developmental Dan Kelainan Mata Pada Anak (Microphtalmia) - RSDDocument5 pagesIT 5 - Visual Developmental Dan Kelainan Mata Pada Anak (Microphtalmia) - RSDIqbal HabibieNo ratings yet
- Case MataDocument2 pagesCase MataIqbal HabibieNo ratings yet
- Per Tanya AnDocument2 pagesPer Tanya AnIqbal HabibieNo ratings yet
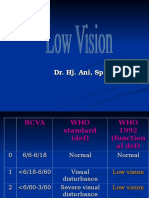
- Low VisionDocument36 pagesLow VisionIqbal HabibieNo ratings yet
- IT 1 - Funduscopic Examination (1) - RZDocument41 pagesIT 1 - Funduscopic Examination (1) - RZIqbal HabibieNo ratings yet
- IT 5 - Visual Developmental Dan Kelainan Mata Pada Anak (Cataract in Children) - RSDDocument21 pagesIT 5 - Visual Developmental Dan Kelainan Mata Pada Anak (Cataract in Children) - RSDIqbal HabibieNo ratings yet
- Organ Transplantation and Protese: DR - Mgs. Roni Saleh, Spb. SPBPDocument22 pagesOrgan Transplantation and Protese: DR - Mgs. Roni Saleh, Spb. SPBPMutia AgustriaNo ratings yet
- IT 7 - Obstetri Fisiologi (Hormon Plasenta) - IZQDocument36 pagesIT 7 - Obstetri Fisiologi (Hormon Plasenta) - IZQIqbal HabibieNo ratings yet
- IT 5 - Gangguan Perkembangan Pervasif (ADHD) - RISDocument15 pagesIT 5 - Gangguan Perkembangan Pervasif (ADHD) - RISIqbal HabibieNo ratings yet
- Facial PalsyDocument12 pagesFacial PalsyIqbal HabibieNo ratings yet
- IT 5 - Visual Developmental Dan Kelainan Mata Pada Anak (Microphtalmia) - RSDDocument5 pagesIT 5 - Visual Developmental Dan Kelainan Mata Pada Anak (Microphtalmia) - RSDIqbal HabibieNo ratings yet
- MCQ It Blok 5Document13 pagesMCQ It Blok 5Iqbal HabibieNo ratings yet
- JADWAL BLOK 8 & Praktikum 2013 RevisiDocument4 pagesJADWAL BLOK 8 & Praktikum 2013 RevisiIqbal HabibieNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Asma AkutDocument8 pagesAsma AkutHayatul ulfaNo ratings yet
- Exercícios: 1. (UNIFOR CE/2006)Document3 pagesExercícios: 1. (UNIFOR CE/2006)erica31No ratings yet
- Asthma and COPD - Basic Mechanisms and Clinical Management 2nd Ed. - P. Barnes, Et. Al., (AP, 2009) WW PDFDocument824 pagesAsthma and COPD - Basic Mechanisms and Clinical Management 2nd Ed. - P. Barnes, Et. Al., (AP, 2009) WW PDFGeorge Danila100% (1)
- A Study On Air and Water Pollution in Sivakasi 3Document28 pagesA Study On Air and Water Pollution in Sivakasi 3dharinipNo ratings yet
- E. DOCK 8 DeficiencyDocument22 pagesE. DOCK 8 DeficiencyAseel AliNo ratings yet
- Mold and Mycotoxins. Effects On The Neurological and Immune SystemsDocument32 pagesMold and Mycotoxins. Effects On The Neurological and Immune Systemsjsenterprises100% (1)
- A Comparative Study of Two Nebulizers in The Emergency Department Breath-Actuated Nebulizer and Handheld NebulizerDocument7 pagesA Comparative Study of Two Nebulizers in The Emergency Department Breath-Actuated Nebulizer and Handheld Nebulizerfachrudin arNo ratings yet
- Perception On The Asthma Amongst Respiratory Therapy StudentsDocument8 pagesPerception On The Asthma Amongst Respiratory Therapy StudentsHeart WpNo ratings yet
- Yuvarajan SMVMCHDocument110 pagesYuvarajan SMVMCHsivagnanameNo ratings yet
- Secrets of Higher ConsciousnessDocument186 pagesSecrets of Higher ConsciousnessRpPaNo ratings yet
- Nawrin JahanDocument82 pagesNawrin JahanMamanya Fadhil HaniNo ratings yet
- Formulation and Evaluation of Time Dependendt Release of Montelukast Tablets by Using Mini Tablet TechnologyDocument13 pagesFormulation and Evaluation of Time Dependendt Release of Montelukast Tablets by Using Mini Tablet TechnologyBaru Chandrasekhar RaoNo ratings yet
- Cannabis Use: Epidemiology, Pharmacology, Comorbidities, and Adverse Effects - UpToDateDocument46 pagesCannabis Use: Epidemiology, Pharmacology, Comorbidities, and Adverse Effects - UpToDateHossdana JimenezNo ratings yet
- DR Julian Whitaker's Unabriged Dictionary of Drug Alternatives and Non-Surgical SolutionsDocument52 pagesDR Julian Whitaker's Unabriged Dictionary of Drug Alternatives and Non-Surgical Solutionsdvtherion100% (1)
- Different Transfer Learning Approaches For Recognition of Lung Sounds ReviewDocument5 pagesDifferent Transfer Learning Approaches For Recognition of Lung Sounds ReviewMeriem HADADJNo ratings yet
- Tyre Fire ReportDocument413 pagesTyre Fire Reportgaza001No ratings yet
- DS FormoterolDocument2 pagesDS FormoterolPang Project100% (1)
- Asthma Control TestDocument1 pageAsthma Control TestRirinBearNo ratings yet
- GINA 2019 Main Report June 2019 Wms PDFDocument201 pagesGINA 2019 Main Report June 2019 Wms PDFAndrada PredaNo ratings yet
- Páginas Desdepharmacotherapy Casebook 10th Ed.Document61 pagesPáginas Desdepharmacotherapy Casebook 10th Ed.Glo VsNo ratings yet
- Bronchiolitis in Infants and Children - Clinical Features and DiagnosisDocument23 pagesBronchiolitis in Infants and Children - Clinical Features and Diagnosisjorgego95No ratings yet
- Dr. Retno Ariza, Sp. P. FCCPDocument40 pagesDr. Retno Ariza, Sp. P. FCCPKaren KuniyaNo ratings yet
- Religiosity On VicesDocument17 pagesReligiosity On VicesJohn Philip ParasNo ratings yet
- Evaluation of Doctor's Knowledge, Attitude, Adherence To Clinical Practice Guideline-Gina 2011 - Recommendarions and Cost Associated With Asthma TreatmentDocument47 pagesEvaluation of Doctor's Knowledge, Attitude, Adherence To Clinical Practice Guideline-Gina 2011 - Recommendarions and Cost Associated With Asthma TreatmentMuhammad IbnRaimyNo ratings yet
- Respiratory System AssignmentDocument3 pagesRespiratory System AssignmentzainaNo ratings yet
- NCPDocument9 pagesNCPEjie Boy Isaga67% (3)
- Lumber Mold - WPPA - Mold-Housing-Wood-Tg2Document12 pagesLumber Mold - WPPA - Mold-Housing-Wood-Tg2Jeff HNo ratings yet
- Cipla announces a new respiratory inhaler: Synchrobreathe (SB), a state-of-the-art breath-actuated inhaler which willbring relief to millions of patients with Obstructive Airway Disease (OAD, asthma and COPD) [Company Update]Document2 pagesCipla announces a new respiratory inhaler: Synchrobreathe (SB), a state-of-the-art breath-actuated inhaler which willbring relief to millions of patients with Obstructive Airway Disease (OAD, asthma and COPD) [Company Update]Shyam SunderNo ratings yet
- Respiratory System QuestionsDocument8 pagesRespiratory System Questionschristine_8995No ratings yet
- Connecting Worlds WorkbookDocument86 pagesConnecting Worlds WorkbookAccessible Journal Media: Peace Corps Documents100% (1)



















































































![Cipla announces a new respiratory inhaler: Synchrobreathe (SB), a state-of-the-art breath-actuated inhaler which willbring relief to millions of patients with Obstructive Airway Disease (OAD, asthma and COPD) [Company Update]](https://imgv2-2-f.scribdassets.com/img/document/274155332/149x198/31f3043092/1439278155?v=1)

