You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Ear Training EssentialsDocument85 pagesEar Training EssentialsJuan Ramiro Pacheco Aguilar100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Daria TV ScriptsDocument1,018 pagesDaria TV ScriptsFrater Bier100% (5)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Chuck Palahniuk: Beyond The Body A Representation of Gender in "Fight Club", "Invisible Monsters" and "Diary" - Kjersti JacbosenDocument115 pagesChuck Palahniuk: Beyond The Body A Representation of Gender in "Fight Club", "Invisible Monsters" and "Diary" - Kjersti JacbosenCamelia PleșaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- MnemonicDocument21 pagesMnemonicWiDya EmiLiaNo ratings yet
- Respiratory Examination: The Position of The PatientDocument24 pagesRespiratory Examination: The Position of The PatientMuhammed Barznji100% (1)
- A. Webern - Drei Kleine Stucke, Op.11 No.1Document22 pagesA. Webern - Drei Kleine Stucke, Op.11 No.1renz_adameNo ratings yet
- Michael: Ginansilyo - Ni - MaryaDocument9 pagesMichael: Ginansilyo - Ni - MaryaCintia Vargas93% (56)
- Analysis of The Okinawan BubishiDocument44 pagesAnalysis of The Okinawan Bubishijerry lee100% (2)
- Clarinet SongsDocument5 pagesClarinet SongsJose Claudio da Silva100% (1)
- 10 Foreign Writers With DescriptionDocument11 pages10 Foreign Writers With DescriptionMyleenx PrlntlngshopNo ratings yet
- The LanguageLab Library - HjfjhfjgfjIELTS Advantage - Speaking and Listening SkillsDocument2 pagesThe LanguageLab Library - HjfjhfjgfjIELTS Advantage - Speaking and Listening SkillsMuhammed BarznjiNo ratings yet
- Road AccidentDocument70 pagesRoad AccidentSakthivel Pachaivel100% (1)
- The LanguageLab Library - 1IELTS Advantage - Speaking and Listening SkillsDocument2 pagesThe LanguageLab Library - 1IELTS Advantage - Speaking and Listening SkillsMuhammed BarznjiNo ratings yet
- DetailedapproaDocument65 pagesDetailedapproaMuhammed BarznjiNo ratings yet
- EpiglottitisDocument2 pagesEpiglottitisMuhammed BarznjiNo ratings yet
- Cranial NervesexaminationanddisordersDocument44 pagesCranial NervesexaminationanddisordersMuhammed BarznjiNo ratings yet
- GTNCVDocument18 pagesGTNCVMuhammed BarznjiNo ratings yet
- Consequences of PrematurityDocument15 pagesConsequences of PrematurityMuhammed BarznjiNo ratings yet
- Early MiscarriageretrjytkuyiulDocument6 pagesEarly MiscarriageretrjytkuyiulMuhammed BarznjiNo ratings yet
- Scora Wad Report v0312Document14 pagesScora Wad Report v0312Muhammed BarznjiNo ratings yet
- Pe Intro PDFDocument39 pagesPe Intro PDFMuhammed BarznjiNo ratings yet
- 10-TCT 2012fyughklDocument196 pages10-TCT 2012fyughklMuhammed BarznjiNo ratings yet
- What Is Gestational Trophoblastic Disease?Document42 pagesWhat Is Gestational Trophoblastic Disease?Muhammed BarznjiNo ratings yet
- Postpartum Hemorrhageghjk,.Document5 pagesPostpartum Hemorrhageghjk,.Muhammed BarznjiNo ratings yet
- Pe AbdominalexamdgfhgjhkDocument20 pagesPe AbdominalexamdgfhgjhkMuhammed BarznjiNo ratings yet
- Local AnestheticsgfhgjhkjlkDocument3 pagesLocal AnestheticsgfhgjhkjlkMuhammed BarznjiNo ratings yet
- Couples With Recurrent MiscarriageDocument18 pagesCouples With Recurrent MiscarriageSimon AhmadpourNo ratings yet
- Crying - Dr. Shwan: Causes?!Document2 pagesCrying - Dr. Shwan: Causes?!Muhammed BarznjiNo ratings yet
- Osce SpeechDocument3 pagesOsce SpeechKai JieNo ratings yet
- Pi An Ectopic PregnancyhjkDocument7 pagesPi An Ectopic PregnancyhjkMuhammed BarznjiNo ratings yet
- Lung & Thorax Exams: Charlie Goldberg, M.D. Professor of Medicine, UCSD SOMDocument33 pagesLung & Thorax Exams: Charlie Goldberg, M.D. Professor of Medicine, UCSD SOMMuhammed BarznjiNo ratings yet
- Cranial Nerve Examination: OverviewDocument8 pagesCranial Nerve Examination: OverviewMuhammed BarznjiNo ratings yet
- Gestational Trop Ho Blastic DiseaseDocument9 pagesGestational Trop Ho Blastic DiseaseMuhammed BarznjiNo ratings yet
- 9220735Document6 pages9220735Muhammed BarznjiNo ratings yet
- Cranial Nerve Examination: OverviewDocument8 pagesCranial Nerve Examination: OverviewMuhammed BarznjiNo ratings yet
- Cerebellar ExaminationDocument1 pageCerebellar ExaminationMuhammed BarznjiNo ratings yet
- Limb Length DiscrepancyDocument2 pagesLimb Length DiscrepancyMuhammed BarznjiNo ratings yet
- Project Camelot David Wilcock (The Road To Ascension) 2007 Transcript - Part 1Document19 pagesProject Camelot David Wilcock (The Road To Ascension) 2007 Transcript - Part 1phasevmeNo ratings yet
- Unit 8: Focus On Time Analysis: - Before You ReadDocument5 pagesUnit 8: Focus On Time Analysis: - Before You ReadScribd0ProfileNo ratings yet
- Work of ArchDocument5 pagesWork of ArchMadhu SekarNo ratings yet
- Present Perfect or Simple Past B-1aDocument2 pagesPresent Perfect or Simple Past B-1aJonny ZamudioNo ratings yet
- The Assumption of The Blessed Virgin MaryDocument21 pagesThe Assumption of The Blessed Virgin MaryPablo FolonierNo ratings yet
- St. Mary's College of Catbalogan: Learning PackageDocument3 pagesSt. Mary's College of Catbalogan: Learning PackageMagdalena BianesNo ratings yet
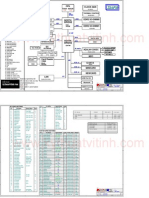
- Asus Z84FMDocument66 pagesAsus Z84FMNicu LiviuNo ratings yet
- Food Revolution Day LyricsDocument1 pageFood Revolution Day LyricsMaría Laura PonzNo ratings yet
- This Is WEG PDFDocument16 pagesThis Is WEG PDFM.DINESH KUMARNo ratings yet
- Submitted To:: Dr. Sarvani VDocument33 pagesSubmitted To:: Dr. Sarvani Vsurbhimo100% (4)
- Book of Forbidden KnowledgeDocument22 pagesBook of Forbidden KnowledgeEmoniel Cutlass59% (131)
- Ss Colonial Newspaper ProjectDocument1 pageSs Colonial Newspaper Projectapi-226792997No ratings yet
- Drinking PDFDocument32 pagesDrinking PDFPencils of PromiseNo ratings yet
- Dental Photography: Camera Equipment!: Dentist BlogDocument5 pagesDental Photography: Camera Equipment!: Dentist BlogNaunit VaidNo ratings yet
- RawPedia BookDocument187 pagesRawPedia BookMike Ignatius Nelson100% (1)
- Local ShoppingDocument2 pagesLocal ShoppingMariangely RamosNo ratings yet
- Noli Me Tangere Past TenseDocument28 pagesNoli Me Tangere Past TenseSan Chez SanchNo ratings yet
- Annotated Bibliography For House Made of DawnDocument6 pagesAnnotated Bibliography For House Made of DawnRam GoliNo ratings yet
- Cuaderno de Verano Ingles 3 Ep PDFDocument16 pagesCuaderno de Verano Ingles 3 Ep PDFAmparo AparisiNo ratings yet
- Neighbourhood PlanningDocument11 pagesNeighbourhood PlanningVidhu Krishna VsNo ratings yet
- Editable Test Unit 2 Challenge LevelDocument4 pagesEditable Test Unit 2 Challenge LevelAlba Lucía Corrales ReinaNo ratings yet
- Curriculum Map ENGLISH 2 Edited PRINTED 1-4Document11 pagesCurriculum Map ENGLISH 2 Edited PRINTED 1-4Jo MeiNo ratings yet