You might also like
- Kuliah Hyper and Hypothyroid - 2014Document66 pagesKuliah Hyper and Hypothyroid - 2014Clararida RiawanNo ratings yet
- Class 6 (19.07.2022)Document70 pagesClass 6 (19.07.2022)Ãqûã FîggâNo ratings yet
- Thyroid Function Tests: Understanding the Hidden Health ProblemDocument34 pagesThyroid Function Tests: Understanding the Hidden Health Problemvjanand07100% (1)
- Thyroid Tests: What Is The Thyroid?Document8 pagesThyroid Tests: What Is The Thyroid?JyotiNo ratings yet
- Endocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Document17 pagesEndocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Ali AlyahawiNo ratings yet
- Thyroid Parathyroid (2012)Document83 pagesThyroid Parathyroid (2012)Hesti AnggrainiNo ratings yet
- The Thyroid Gland and ProblemsDocument12 pagesThe Thyroid Gland and ProblemsLeslie PaguioNo ratings yet
- Semen, Thyroid, Renal and Liver Function Tests InterpretationDocument38 pagesSemen, Thyroid, Renal and Liver Function Tests Interpretationdeepika bananiNo ratings yet
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- Disorders of the Thyroid: A Guide to Diagnosis and TreatmentDocument36 pagesDisorders of the Thyroid: A Guide to Diagnosis and TreatmentMita Erna WatiNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document8 pagesThyroid Function Tests: What Is The Thyroid Gland?Rahadiyan HadinataNo ratings yet
- Interpreting Thyroid Tests: Key FactorsDocument7 pagesInterpreting Thyroid Tests: Key FactorsStrawberry ShortcakeNo ratings yet
- Thyroid Function Tests and Goitre SV 24-4-21Document51 pagesThyroid Function Tests and Goitre SV 24-4-21Lal KhanNo ratings yet
- Thyroid DisordersDocument22 pagesThyroid DisordersNimer Abdelhadi AliNo ratings yet
- Clinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismDocument69 pagesClinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismTutde SedanaNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document2 pagesThyroid Function Tests: What Is The Thyroid Gland?rastamaneazy269No ratings yet
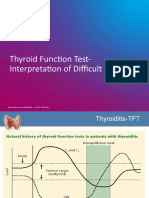
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- Thyroid Function Test (TFT'S) : Presented By: Shoaib Ahmad Usama Maqsood Kamran AnjumDocument52 pagesThyroid Function Test (TFT'S) : Presented By: Shoaib Ahmad Usama Maqsood Kamran AnjumpriyaNo ratings yet
- Hypothyroidism in PregnancyDocument32 pagesHypothyroidism in PregnancyNicks KumarNo ratings yet
- Thyroid Function TestDocument11 pagesThyroid Function TestBookmyscansNo ratings yet
- Thyroid Disorders: Dr. Lubna DwerijDocument52 pagesThyroid Disorders: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyNo ratings yet
- Diagnosis and Evaluation of Thyroid DisordersDocument21 pagesDiagnosis and Evaluation of Thyroid DisordersIvan AditamaNo ratings yet
- Biochemical Testing of The Thyroid: TSH Is The Best And, Oftentimes, Only Test Needed - A Review For Primary CareDocument10 pagesBiochemical Testing of The Thyroid: TSH Is The Best And, Oftentimes, Only Test Needed - A Review For Primary CareElsaBorrellGarcíaNo ratings yet
- Thyroid Function TestDocument2 pagesThyroid Function Testhannah lanasaNo ratings yet
- Thyroid Function TestDocument31 pagesThyroid Function TestMeno AliNo ratings yet
- AACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismDocument63 pagesAACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismNur Rakhma AkmaliaNo ratings yet
- Thyroid Function and Phytotherapy - Rosalind BlackwellDocument14 pagesThyroid Function and Phytotherapy - Rosalind BlackwellCPP-libraryNo ratings yet
- 0a27thyroid Function TestDocument35 pages0a27thyroid Function TestAshokvardhan Chowdary Nandigam67% (3)
- ThyrotoxicosisDocument105 pagesThyrotoxicosisAli Murtaza Abbas100% (1)
- Interpretation of Laboratory Thyroid Function Tests: The "Hidden" Health ProblemDocument38 pagesInterpretation of Laboratory Thyroid Function Tests: The "Hidden" Health Problemalanoud.877No ratings yet
- Gangguan Struktur & Fungsi EndokrinDocument63 pagesGangguan Struktur & Fungsi EndokrinLaurensia MassariNo ratings yet
- Thyroid Disease: Posted by Christiane Northrup, M.DDocument17 pagesThyroid Disease: Posted by Christiane Northrup, M.DSathishNo ratings yet
- Thyroid Talk-FMD RdsDocument58 pagesThyroid Talk-FMD RdsSriman YarrarapuNo ratings yet
- Thyroid Function and Disease: Sponsored by Department of Continuing Medical EducationDocument69 pagesThyroid Function and Disease: Sponsored by Department of Continuing Medical EducationSriman YarrarapuNo ratings yet
- OBAT HIPOTIROID dan HIPERTIROIDDocument30 pagesOBAT HIPOTIROID dan HIPERTIROIDRhandy SeptiantoNo ratings yet
- Thyroid Function, Levels and Disorders ExplainedDocument46 pagesThyroid Function, Levels and Disorders ExplainedsinayupeNo ratings yet
- Stop The Thyroid Madness Sanjay Dixit MDDocument68 pagesStop The Thyroid Madness Sanjay Dixit MDdb50% (2)
- FunctionTests BrochureDocument2 pagesFunctionTests Brochurejonalyntonato09No ratings yet
- Thyroid Disorders Guide: Causes, Symptoms & TreatmentsDocument81 pagesThyroid Disorders Guide: Causes, Symptoms & Treatmentschetankumarbhumireddy50% (2)
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Risk For Progression To Overt Hypothyroidism in An Elderly Japanese Population With Subclinical HypothyroidismDocument6 pagesRisk For Progression To Overt Hypothyroidism in An Elderly Japanese Population With Subclinical HypothyroidismJavier Burgos CárdenasNo ratings yet
- Thyroid Tests and ResultsDocument9 pagesThyroid Tests and ResultsKristel BelgicaNo ratings yet
- Thyroid Function Tests PPT of IMS BHUDocument74 pagesThyroid Function Tests PPT of IMS BHUPriyanshu Mandal100% (1)
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocument5 pagesHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaNo ratings yet
- TSH Test: Alkitab University - Collage of Medical Techniques Department of Medical AnalysisDocument4 pagesTSH Test: Alkitab University - Collage of Medical Techniques Department of Medical AnalysisAhmed AhmedNo ratings yet
- Hyperthyroidism With Signs and Symptoms of Thyrotoxicosis: A Case Protocol OnDocument6 pagesHyperthyroidism With Signs and Symptoms of Thyrotoxicosis: A Case Protocol Onscremo_xtremeNo ratings yet
- Tiroid 2012Document27 pagesTiroid 2012Amali FikriahNo ratings yet
- #30 Thyroid and Thyroid TestingDocument25 pages#30 Thyroid and Thyroid TestingasclswisconsinNo ratings yet
- Thyroid Function TestsDocument21 pagesThyroid Function TestsPraneeth TirumalasettyNo ratings yet
- THYROID FUNCTION TESTS DSL PACKAGEDocument7 pagesTHYROID FUNCTION TESTS DSL PACKAGEUmar AzlanNo ratings yet
- Investigating Low TSH (BMJ 2013) Endocrine DisordersDocument4 pagesInvestigating Low TSH (BMJ 2013) Endocrine DisordersLouiseNo ratings yet
- Module I 2 - Thyroid Gland DisordersDocument43 pagesModule I 2 - Thyroid Gland Disordersaysha jasimNo ratings yet
- An Analytical Study of Thyroid Hormones in Different Temperaments (Mizaj)Document7 pagesAn Analytical Study of Thyroid Hormones in Different Temperaments (Mizaj)yusufNo ratings yet
- Thyroid HormonesDocument63 pagesThyroid HormonesDr. M. Prasad NaiduNo ratings yet
- TSH Levels Low To High Ranges, Symptoms, and WhaDocument1 pageTSH Levels Low To High Ranges, Symptoms, and WhaErwin Dela GanaNo ratings yet
- The Thyroid, Cancer and You: Knowledge Is Power! How Much Do You Know?From EverandThe Thyroid, Cancer and You: Knowledge Is Power! How Much Do You Know?No ratings yet
- Thyroid Dse - SupersummaryDocument3 pagesThyroid Dse - SupersummaryMissDyYournurseNo ratings yet
- Reflective EssayDocument5 pagesReflective Essayjessicadietlin100% (1)
- SENSORY ORGANS: ANIMAL PERCEPTIONDocument19 pagesSENSORY ORGANS: ANIMAL PERCEPTIONWE ARE CRaZyNo ratings yet
- 5 Sore ThroatDocument45 pages5 Sore ThroatNurul Wandasari SNo ratings yet
- 30 Best Curly Hairstyles For Medium Hair - BelleTagDocument1 page30 Best Curly Hairstyles For Medium Hair - BelleTagJamaica Kim JimenezNo ratings yet
- Effectiveness of The Canalith Repositioning Procedure in The Treatment of Benign Paroxysmal Positional VertigoDocument11 pagesEffectiveness of The Canalith Repositioning Procedure in The Treatment of Benign Paroxysmal Positional VertigoNia UtariNo ratings yet
- Cleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishraDocument9 pagesCleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishranomanNo ratings yet
- Biomechanics of Head GearDocument33 pagesBiomechanics of Head GearLipika Mali100% (1)
- Jurnal Kasus Tambahan 3 - Khairin Yonni (12730)Document6 pagesJurnal Kasus Tambahan 3 - Khairin Yonni (12730)Khairin YonniNo ratings yet
- Appearance Vocabulary Exercises Fun Activities Games Icebreakers Oneonone Activiti - 46320Document2 pagesAppearance Vocabulary Exercises Fun Activities Games Icebreakers Oneonone Activiti - 46320Olinda Lopez67% (3)
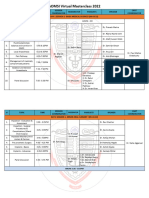
- AOMSI MC2022 ScheduleDocument10 pagesAOMSI MC2022 ScheduleDarain ShahidNo ratings yet
- Golden Key PointsDocument8 pagesGolden Key PointsBijay Kumar MahatoNo ratings yet
- Cleft Lip and Palate GuideDocument4 pagesCleft Lip and Palate GuideMaricel DefiestaNo ratings yet
- Common Ent EmergenciesDocument65 pagesCommon Ent EmergenciesferaNo ratings yet
- Ipdoaj MS Id 000113Document3 pagesIpdoaj MS Id 000113Ayu DamayNo ratings yet
- Acupressure Points To Relieve Jaw TensionDocument4 pagesAcupressure Points To Relieve Jaw TensionsunsignNo ratings yet
- CVS, Respi Heent ExamDocument8 pagesCVS, Respi Heent ExamDranreb Berylle MasangkayNo ratings yet
- Examination of Lacrimal ApparatusDocument23 pagesExamination of Lacrimal ApparatusDr. T. BalasubramanianNo ratings yet
- Human Eye PDFDocument13 pagesHuman Eye PDFHaidir MuhammadNo ratings yet
- Hsieh - Nuance in Bilateral Cleft Lip RepairDocument9 pagesHsieh - Nuance in Bilateral Cleft Lip RepairFauzia Latifah SupriyadiNo ratings yet
- Gingival Phenotypes in Young Male Adults: Dinical PenodoiitdiojiyDocument8 pagesGingival Phenotypes in Young Male Adults: Dinical PenodoiitdiojiyValery V JaureguiNo ratings yet
- Median (Third) Occipital CondyleDocument4 pagesMedian (Third) Occipital Condylespin_echoNo ratings yet
- Embryology Finals ReviewDocument53 pagesEmbryology Finals ReviewNdor BariboloNo ratings yet
- Cephalometric Study of Alterations Induced by Maxillary Slow Expansion in Adults PDFDocument7 pagesCephalometric Study of Alterations Induced by Maxillary Slow Expansion in Adults PDFDonald Stephen Florez GuerreroNo ratings yet
- Katalog MB - PPGDocument20 pagesKatalog MB - PPGHerlina SalimNo ratings yet
- Sensory and Motor Cranial NervesDocument13 pagesSensory and Motor Cranial NervesAnn HeerahNo ratings yet
- Mastoiditis Treatment & ManagementDocument10 pagesMastoiditis Treatment & ManagementIvan PathfinderNo ratings yet
- Mandibular Anatomical LandmarksDocument51 pagesMandibular Anatomical LandmarksNishu PriyaNo ratings yet
- Laserx60 enDocument14 pagesLaserx60 enqwertyjinNo ratings yet
- Adult Neurological ExaminationDocument57 pagesAdult Neurological ExaminationSandeep Soni100% (1)