You might also like
- Pelvis and HipDocument90 pagesPelvis and Hipalsead798No ratings yet
- Pelvic TraumaDocument20 pagesPelvic Traumachehak.kumar2000No ratings yet
- Pelvic InjuriesDocument35 pagesPelvic InjuriesJavier Saad100% (1)
- Pelvic Fractures PksDocument48 pagesPelvic Fractures PksprinceveettoorNo ratings yet
- Potentially Life-Threatening Extremity InjuriesDocument41 pagesPotentially Life-Threatening Extremity Injuriesyuliaoksiyulanda ingeniopadangNo ratings yet
- Pelvic Injruies 2Document57 pagesPelvic Injruies 2King salehNo ratings yet
- Case Report: Rehabilitation Program in A Patient With Congenital Dysplasia and Subluxation of The HipDocument26 pagesCase Report: Rehabilitation Program in A Patient With Congenital Dysplasia and Subluxation of The HipNatalia LoredanaNo ratings yet
- Lapsus Ortho Word - Id.enDocument17 pagesLapsus Ortho Word - Id.eninhaNo ratings yet
- Pelvic FractureDocument18 pagesPelvic FractureTantyaNo ratings yet
- Pelvic Injury (Autosaved)Document44 pagesPelvic Injury (Autosaved)abhishek chaudharyNo ratings yet
- SPONDYLOLISTHESISDocument50 pagesSPONDYLOLISTHESISAnuj ShresthaNo ratings yet
- Tuberculosis of Hip JointDocument25 pagesTuberculosis of Hip JointYousra ShaikhNo ratings yet
- Pelvic Trauma: Stud.: Andris Džeriņš, MF V 5.gr. Mentor: Dr. Med. Ruta JakušonokaDocument46 pagesPelvic Trauma: Stud.: Andris Džeriņš, MF V 5.gr. Mentor: Dr. Med. Ruta JakušonokaRendy SusantoNo ratings yet
- Dislokasi Panggul & BahuDocument42 pagesDislokasi Panggul & BahuAnton TrihartantoNo ratings yet
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDocument97 pagesHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyNo ratings yet
- Bilateral Inter-Faceted Dislocation of Cervical Spine: Closed Reduction With Traction Weights - Small and Slow or Lose It All (Neurology)Document10 pagesBilateral Inter-Faceted Dislocation of Cervical Spine: Closed Reduction With Traction Weights - Small and Slow or Lose It All (Neurology)ICNo ratings yet
- Hip DislocDocument67 pagesHip DislocAli TawbeNo ratings yet
- Pelvic Injruies 1Document43 pagesPelvic Injruies 1King salehNo ratings yet
- Materi Kuliah FK ULM 2022 - Lower Extremity I - Hip & KneeDocument61 pagesMateri Kuliah FK ULM 2022 - Lower Extremity I - Hip & Kneezaki ridhoniNo ratings yet
- Methas Arunnart MDDocument38 pagesMethas Arunnart MDjackie funtanillaNo ratings yet
- Rotator Cuff InjuryDocument29 pagesRotator Cuff InjuryArko duttaNo ratings yet
- Anks PondDocument32 pagesAnks Pondmiskiah lainunNo ratings yet
- Dislocations (PDFDrive)Document111 pagesDislocations (PDFDrive)hemasary15No ratings yet
- Ortho Review 1Document67 pagesOrtho Review 1mark tNo ratings yet
- Pelvictrauma 151103203943 Lva1 App6892Document40 pagesPelvictrauma 151103203943 Lva1 App6892Navin BalajiNo ratings yet
- Hip Disloc and Fem HeadDocument60 pagesHip Disloc and Fem HeadZisuhNo ratings yet
- Orthopedic Conditions in PaedsDocument57 pagesOrthopedic Conditions in PaedsAsma AlamNo ratings yet
- Cervical Spine AnatomyDocument67 pagesCervical Spine AnatomyAnonymous glhczXqdDNo ratings yet
- Untitled PresentationDocument44 pagesUntitled PresentationMika PamulangNo ratings yet
- Treatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisDocument5 pagesTreatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisPeko PekoNo ratings yet
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Talar Fracture Repair and RehabilitationDocument4 pagesTalar Fracture Repair and RehabilitationAlexandra NadinneNo ratings yet
- FR dISLOKASI BAHUDocument39 pagesFR dISLOKASI BAHUnurul azizaNo ratings yet
- C2 Chordoma A Case Report: Dr. M. Ashok Kumar Consultant Spine Surgeon, SNHRC, VelloreDocument38 pagesC2 Chordoma A Case Report: Dr. M. Ashok Kumar Consultant Spine Surgeon, SNHRC, VellorevarshneyNo ratings yet
- HIP JOINT Special Tests-WPS OfficeDocument51 pagesHIP JOINT Special Tests-WPS OfficeManisha MishraNo ratings yet
- 08 - Khansa Qonita R - Case ReportDocument15 pages08 - Khansa Qonita R - Case Reportarif yogi0% (1)
- Pelvic Fractures ManagementDocument24 pagesPelvic Fractures ManagementSerenna DehalooNo ratings yet
- Document 85Document51 pagesDocument 85Shameena AnwarNo ratings yet
- Shoulder Dislocation: Orthopedics Department DR Kilian K.KDocument32 pagesShoulder Dislocation: Orthopedics Department DR Kilian K.KInnocentNo ratings yet
- Manajemen Fraktur PelvisDocument30 pagesManajemen Fraktur PelvisNadya Wiratami NurrakhmawatiNo ratings yet
- Anterior Knee Pain Syndrome ReferatDocument28 pagesAnterior Knee Pain Syndrome ReferatnurulNo ratings yet
- Kyphosis Physiotherapy From Childhood To Old Age: Jean Claude de MauroyDocument26 pagesKyphosis Physiotherapy From Childhood To Old Age: Jean Claude de MauroyromanciviNo ratings yet
- Pelvic FractureDocument89 pagesPelvic FractureAndreas RendraNo ratings yet
- Pelvic FractureDocument31 pagesPelvic Fracturepoe3No ratings yet
- CR - RamirezDocument4 pagesCR - RamirezTommysNo ratings yet
- Fracture-Dislocation of The Hip-KaizarDocument69 pagesFracture-Dislocation of The Hip-KaizarKaizar Ennis100% (1)
- Fracture Pelvis, Hip DislocationsDocument34 pagesFracture Pelvis, Hip DislocationsMisoNo ratings yet
- Family Medicine DepartmentDocument45 pagesFamily Medicine Departmentسليمان فايزNo ratings yet
- FIU - Cervical SpineDocument42 pagesFIU - Cervical Spineamoon12No ratings yet
- 20.nyeri PunggungDocument53 pages20.nyeri PunggungAy'oe Ithyu RezthuNo ratings yet
- Acetabular FractureDocument136 pagesAcetabular FracturePicha PichiNo ratings yet
- Initial Management in Musculoskeletal Trauma: Yoyos D. IsmiartoDocument40 pagesInitial Management in Musculoskeletal Trauma: Yoyos D. IsmiartozaroziNo ratings yet
- Acetabular and Hip FractureDocument133 pagesAcetabular and Hip FractureJuanita HenryNo ratings yet
- Hip DislocationDocument39 pagesHip DislocationSHAMENI VINODNo ratings yet
- Pelvic Fractures: Part 1. Evaluation, Classification, and ResuscitationDocument28 pagesPelvic Fractures: Part 1. Evaluation, Classification, and ResuscitationRiven OktavianNo ratings yet
- DISH y Calcificacion Del LLPDocument5 pagesDISH y Calcificacion Del LLPRODALLIENDENo ratings yet
- Advance Trauma Life Support: Andi Siswandi, MD Surgeon Malahayati University, Medicine FacultyDocument76 pagesAdvance Trauma Life Support: Andi Siswandi, MD Surgeon Malahayati University, Medicine Facultyhari dorismanNo ratings yet
- Adhesive CapsulitisDocument20 pagesAdhesive Capsulitisvenkata ramakrishnaiahNo ratings yet
- Leadership 1 EntrepreneurDocument37 pagesLeadership 1 EntrepreneurRsud Malinau Ppk BludNo ratings yet
- III. Dr. Imran - MZ ARIFINIMRAN Coagulopathy and Head InjuryDocument36 pagesIII. Dr. Imran - MZ ARIFINIMRAN Coagulopathy and Head InjuryRsud Malinau Ppk BludNo ratings yet
- III - Dr. Imran - Severe Head Injury, Trauma Update XIIDocument22 pagesIII - Dr. Imran - Severe Head Injury, Trauma Update XIIRsud Malinau Ppk BludNo ratings yet
- Dr. Kiki - Pengantar Trauma UpdateDocument20 pagesDr. Kiki - Pengantar Trauma UpdateRsud Malinau Ppk Blud100% (1)
- B. Dr. Yoyos D. I - Traumatic Crush Syndromejam13Document28 pagesB. Dr. Yoyos D. I - Traumatic Crush Syndromejam13Rsud Malinau Ppk BludNo ratings yet
- I. Dr. Noer. Case Fracture PelvisDocument7 pagesI. Dr. Noer. Case Fracture PelvisRsud Malinau Ppk BludNo ratings yet
- Dr. Setyorini - Trauma Update 2014Document38 pagesDr. Setyorini - Trauma Update 2014Rsud Malinau Ppk BludNo ratings yet
- Dr. Yoyos - Acute Cervical Injury FinalDocument30 pagesDr. Yoyos - Acute Cervical Injury FinalRsud Malinau Ppk BludNo ratings yet
- Dr. Kiki - Lecture 1 - Update Management of Hemorrhagic Shock & Traumatic Coagulopathy-KikiDocument20 pagesDr. Kiki - Lecture 1 - Update Management of Hemorrhagic Shock & Traumatic Coagulopathy-KikiRsud Malinau Ppk BludNo ratings yet
- DR - Noer Rachmat Early Management Pelvic FractureDocument72 pagesDR - Noer Rachmat Early Management Pelvic FractureRsud Malinau Ppk BludNo ratings yet
- Dr. Lisa PPT Burn Injury Revisi OkDocument35 pagesDr. Lisa PPT Burn Injury Revisi OkRsud Malinau Ppk BludNo ratings yet
- Dr. Yoyos - Acute Cervical Injury FinalDocument30 pagesDr. Yoyos - Acute Cervical Injury FinalRsud Malinau Ppk BludNo ratings yet
- Dr. Kiki Update On DCR and DCSDocument39 pagesDr. Kiki Update On DCR and DCSRsud Malinau Ppk Blud100% (1)
- Dr. Rama - Torakotomi Pada Trauma 2dr. RamaDocument65 pagesDr. Rama - Torakotomi Pada Trauma 2dr. RamaRsud Malinau Ppk BludNo ratings yet
- Strategi Rs Di Era JKNDocument45 pagesStrategi Rs Di Era JKNRsud Malinau Ppk BludNo ratings yet
- Accountability SystemDocument44 pagesAccountability SystemRsud Malinau Ppk BludNo ratings yet
- SBP PNP Analysis PDFDocument3 pagesSBP PNP Analysis PDFAlexavier DylanNo ratings yet
- Breastfeeding PDFDocument11 pagesBreastfeeding PDFSatya Prakash TiwariNo ratings yet
- 100 Gross Anatomy ConceptionsDocument228 pages100 Gross Anatomy Conceptionscrsoriano2011No ratings yet
- 2nd Announcement ACA2015Document16 pages2nd Announcement ACA2015Dimas Rangga WNo ratings yet
- PedsQL Scoring PDFDocument146 pagesPedsQL Scoring PDFRam Pokharel100% (1)
- NCP For Acvute PainDocument6 pagesNCP For Acvute PainGlenn ValerioNo ratings yet
- Reflective EssayDocument5 pagesReflective Essayjessicadietlin100% (1)
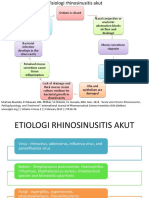
- THT RhinosinusitisDocument8 pagesTHT RhinosinusitismeiliaNo ratings yet
- PRC Forms Bicol University COllege of Nursing, Legazpi CityDocument5 pagesPRC Forms Bicol University COllege of Nursing, Legazpi CityekagaliasNo ratings yet
- Paracetamol A Review of Three Routes of AdministrationDocument3 pagesParacetamol A Review of Three Routes of AdministrationMohd MiqdamNo ratings yet
- Vicorder PWA-PWV Pres 15-04 EnglDocument79 pagesVicorder PWA-PWV Pres 15-04 EnglHatem FaroukNo ratings yet
- Funds FlowDocument78 pagesFunds FlowSaisanthosh Kumar SharmaNo ratings yet
- E-Book - Basic Concepts of PharmacokineticsDocument71 pagesE-Book - Basic Concepts of PharmacokineticsCryslene VenancioNo ratings yet
- Orgasmic Birth Review5Document2 pagesOrgasmic Birth Review5Bnaren NarenNo ratings yet
- TetanusDocument6 pagesTetanusAflah Dhea Bariz YastaNo ratings yet
- Student Guide: SourceDocument82 pagesStudent Guide: Sourcewaraney palitNo ratings yet
- High-Dose Methotrexate, Leucovorin and Glucarpidase Dosing, Administration, and Monitoring - Adult/Pediatric - Inpatient Clinical Practice GuidelineDocument15 pagesHigh-Dose Methotrexate, Leucovorin and Glucarpidase Dosing, Administration, and Monitoring - Adult/Pediatric - Inpatient Clinical Practice GuidelineKena BenNo ratings yet
- Institute of Neurosciences Kolkata (Schedule) PDFDocument2 pagesInstitute of Neurosciences Kolkata (Schedule) PDFpvkdasaNo ratings yet
- Neurological AssessmentDocument47 pagesNeurological AssessmentRian TheredNo ratings yet
- Molar Access Dcna 1Document26 pagesMolar Access Dcna 1mahmoudNo ratings yet
- Ansiedad y GastritisDocument5 pagesAnsiedad y Gastritisjose fernandezNo ratings yet
- 1 4994706266967244834 PDFDocument497 pages1 4994706266967244834 PDFWilfredo Cvanegas75% (4)
- Notification No. SO (SC) 1-13317 Seniority List of Consultants (BS-18) 1-3-18Document51 pagesNotification No. SO (SC) 1-13317 Seniority List of Consultants (BS-18) 1-3-18IrfanNo ratings yet
- Symposium Brochure Bronx HeartDocument12 pagesSymposium Brochure Bronx Heartyos_peace86No ratings yet
- Daftar PustakaDocument12 pagesDaftar PustakaRenata YolandaNo ratings yet
- Fluoride and The Oral Environment PDFDocument190 pagesFluoride and The Oral Environment PDFMagyari AttilaNo ratings yet
- Studyindia: Neet PG Admissions Seat Matrix, Fee Structure and Cut-OffDocument25 pagesStudyindia: Neet PG Admissions Seat Matrix, Fee Structure and Cut-OffSARKAR JAVED AKHTARNo ratings yet
- Bladder Outlet Obstruction in Children PDFDocument64 pagesBladder Outlet Obstruction in Children PDFalaaNo ratings yet
- Andre Tan's Surgery Notes (Ed 1)Document163 pagesAndre Tan's Surgery Notes (Ed 1)Daniel LimNo ratings yet
- Ainsworth Bowlby 1Document1 pageAinsworth Bowlby 1jasonNo ratings yet