You might also like
- Report PhysioRes 1Document3 pagesReport PhysioRes 1Said Taysir AbdlJawadNo ratings yet
- Ventilation Perfusion MatchingDocument4 pagesVentilation Perfusion Matchingrroo3No ratings yet
- Abnormal Ventilation, Abnormal Gas ExchangeDocument52 pagesAbnormal Ventilation, Abnormal Gas ExchangekateNo ratings yet
- Acute Respiratory Fauilr - PDF CVS PART 4Document61 pagesAcute Respiratory Fauilr - PDF CVS PART 4LexNo ratings yet
- V/Q and Oxygen: Anuja Abayadeera Part 1B AnaesthsiologyDocument42 pagesV/Q and Oxygen: Anuja Abayadeera Part 1B Anaesthsiologyv_vijayakanth7656No ratings yet
- Respiratory Failure: Lack of Respiratory SuccessDocument41 pagesRespiratory Failure: Lack of Respiratory SuccessYS NateNo ratings yet
- Interpretasi Agd Juni 2020Document34 pagesInterpretasi Agd Juni 2020Christiana TrijayantiNo ratings yet
- Oxygenation and Oxygen TherapyDocument11 pagesOxygenation and Oxygen TherapyJenn77x1No ratings yet
- 2nd Year Respiratory Phys-252807Document17 pages2nd Year Respiratory Phys-252807Christopher WytherNo ratings yet
- Interpretation of Arterial Blood Gases and Acid-Base DisordersDocument44 pagesInterpretation of Arterial Blood Gases and Acid-Base DisordersSuren VishvanathNo ratings yet
- VQ - O2 GradientDocument27 pagesVQ - O2 GradientIkbal NurNo ratings yet
- Oxygen Therapy: Dr. Rajesh AroraDocument59 pagesOxygen Therapy: Dr. Rajesh ArorarkdivyaNo ratings yet
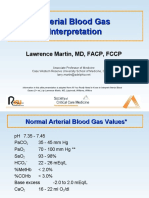
- Arterial Blood Gas InterpretationDocument66 pagesArterial Blood Gas InterpretationlenafitriyaniNo ratings yet
- Arterial Blood Gas InterpretationDocument65 pagesArterial Blood Gas InterpretationDaniel AryanNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Respiratory Physiology: Dr. Okon MRCSDocument41 pagesRespiratory Physiology: Dr. Okon MRCSEdwin OkonNo ratings yet
- Ventilasi PerfusiDocument44 pagesVentilasi PerfusiIdahrachman515100% (1)
- Respiratory FailureDocument38 pagesRespiratory Failuredrmithil100% (1)
- Respiratory Failure Type 1Document15 pagesRespiratory Failure Type 1lady birdNo ratings yet
- Med Lecture - Causes of HypoxemiaDocument6 pagesMed Lecture - Causes of HypoxemiaZoherNBezantiNo ratings yet
- Respiratory ModalitiesDocument87 pagesRespiratory ModalitiesLj Ferolino100% (2)
- Arterial Blood Gas InterpretationDocument66 pagesArterial Blood Gas InterpretationkabatchinoooNo ratings yet
- Hypoxia: Moderator: DR Meera Balasubramanyam Professor Dept of Anaesthesiology MMCRI Speaker: DR Nandhini.K.S.KaratDocument65 pagesHypoxia: Moderator: DR Meera Balasubramanyam Professor Dept of Anaesthesiology MMCRI Speaker: DR Nandhini.K.S.KaratAnn Susan MathewNo ratings yet
- AbgDocument66 pagesAbgIan OrwaNo ratings yet
- Acure Resp Failure and ARDS 1-13-2020Document37 pagesAcure Resp Failure and ARDS 1-13-2020slatcheshotmail.comNo ratings yet
- Ventilation: Describe Alveolar and Pulmonary VentilationDocument6 pagesVentilation: Describe Alveolar and Pulmonary VentilationNorrifhan Akmal IsmailNo ratings yet
- Hanan Fathy Pediatric Nephrology UnitDocument59 pagesHanan Fathy Pediatric Nephrology UnitdrhananfathyNo ratings yet
- Resp InsuffDocument30 pagesResp InsuffCLEMENTNo ratings yet
- (RS) Pneumonia With Severe HypoxiaDocument4 pages(RS) Pneumonia With Severe Hypoxiaapi-3769252100% (2)
- Acute Respiratory Failure - Respina 2010Document25 pagesAcute Respiratory Failure - Respina 2010Agus Dwi SiswantoNo ratings yet
- Chapter 41, Pages 527-537: Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsDocument46 pagesChapter 41, Pages 527-537: Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsAlia HaiderNo ratings yet
- Arterial Blood Gas InterpretationDocument69 pagesArterial Blood Gas InterpretationostuffeNo ratings yet
- Arterial Blood Gases (ABG) : Shaza AlyDocument56 pagesArterial Blood Gases (ABG) : Shaza AlyaymenNo ratings yet
- 15, 16, and 17 - Respiratorio 2011Document86 pages15, 16, and 17 - Respiratorio 2011Redes HostNo ratings yet
- Respiratory ICU PDFDocument130 pagesRespiratory ICU PDFAhmed Shihab AhmedNo ratings yet
- Respiratory Lecture 2 (1 Slide Per Page)Document33 pagesRespiratory Lecture 2 (1 Slide Per Page)AnshikaNo ratings yet
- Common Causes of HypoxemiaDocument6 pagesCommon Causes of HypoxemiaSamantha LuiNo ratings yet
- Oxygen Therapy: Dr. Subhankar ChatterjeeDocument49 pagesOxygen Therapy: Dr. Subhankar ChatterjeesubhankarNo ratings yet
- ABG QuizDocument13 pagesABG QuizSSNo ratings yet
- Respiratory Failure in Children PDFDocument47 pagesRespiratory Failure in Children PDFOxana TurcuNo ratings yet
- Arterial Blood Gases: A Step by Step GuideDocument19 pagesArterial Blood Gases: A Step by Step GuideKathleen Ann50% (2)
- ABG InterpretationDocument38 pagesABG Interpretationmahmod omerNo ratings yet
- Respiratory FailureDocument7 pagesRespiratory FailureJesse OnealNo ratings yet
- Pulmonary Function TestsDocument35 pagesPulmonary Function Testsnirilib100% (4)
- Mechanical VentilationDocument62 pagesMechanical Ventilationdrphaninadella100% (1)
- Oxygen Cascade - SHANTHINIDocument57 pagesOxygen Cascade - SHANTHINIMani BharathiNo ratings yet
- Oxygen Therapy: Prof. Dr. Ioana GrigorașDocument109 pagesOxygen Therapy: Prof. Dr. Ioana GrigorașAna-Maria Croitoru100% (1)
- Ventilation Perfusion RatioDocument13 pagesVentilation Perfusion Ratiojane elizabethNo ratings yet
- ABGs - Oxygen TherapyDocument4 pagesABGs - Oxygen TherapyPebblesNo ratings yet
- Approach To A Hypoxic Patient in IcuDocument64 pagesApproach To A Hypoxic Patient in IcusanjibNo ratings yet
- Arterial Blood GasDocument255 pagesArterial Blood GasMark Joshua S CruzNo ratings yet
- ARDS With PathophysiologyDocument79 pagesARDS With Pathophysiologymabec pagaduan95% (19)
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Lung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyFrom EverandLung Function in Health and Disease Basic Concepts of Respiratory Physiology and PathophysiologyNo ratings yet
- The Spleen: Schwartz's Principles of Surgery 11th EdDocument54 pagesThe Spleen: Schwartz's Principles of Surgery 11th EdaddelinsNo ratings yet
- Myocardial PerfusionDocument169 pagesMyocardial PerfusionUrpy Imperio Morales Morales100% (1)
- Management of Pruritus in Indian Settings: An Expert OpinionDocument13 pagesManagement of Pruritus in Indian Settings: An Expert OpinionJon SnowNo ratings yet
- ENZYMES OF CLINICAL IMPORTANCE ChapterDocument18 pagesENZYMES OF CLINICAL IMPORTANCE ChapterKeerthy VasanNo ratings yet
- Marfan SyndromeDocument19 pagesMarfan SyndromePapp ZselykeNo ratings yet
- 2.2 - All Worksheets - Homework Sheets - Extension SheetsDocument20 pages2.2 - All Worksheets - Homework Sheets - Extension SheetslogineNo ratings yet
- 9region 170425213100Document12 pages9region 170425213100Ashraf SidrahNo ratings yet
- CVS ExaminationDocument72 pagesCVS ExaminationPrashanthBhatNo ratings yet
- Review MSDocument8 pagesReview MSPatrycyaNo ratings yet
- Daftar Diagnosis Dan Kode BPJSDocument18 pagesDaftar Diagnosis Dan Kode BPJSeginagirsangNo ratings yet
- Nursing Test 4 (NP Iii)Document16 pagesNursing Test 4 (NP Iii)Yuxin Liu100% (2)
- COVID-19 - Vaccine - AstraZeneca - UK - Vaccine Analysis Print 24 Nov 2022Document132 pagesCOVID-19 - Vaccine - AstraZeneca - UK - Vaccine Analysis Print 24 Nov 2022Mary-Jane StevensNo ratings yet
- HypomagnesemiaDocument3 pagesHypomagnesemiaapi-3712326No ratings yet
- Pathophysiology: Cardiovascular Diseases Coronary Artery Disease (CAD)Document5 pagesPathophysiology: Cardiovascular Diseases Coronary Artery Disease (CAD)Grace Bernadine H. Ramos100% (1)
- Standards of Care in Diabetes-2024: 4. Comprehensive Medical Evaluation and Assessment of ComorbiditiesDocument25 pagesStandards of Care in Diabetes-2024: 4. Comprehensive Medical Evaluation and Assessment of Comorbiditiesph15027No ratings yet
- SpirometryDocument47 pagesSpirometrydrmahayousif7451100% (2)
- Basic Sciences QN PaperDocument29 pagesBasic Sciences QN PapermanorasmanthewNo ratings yet
- Abg Analysis and InterpretationDocument27 pagesAbg Analysis and InterpretationvaishnaviNo ratings yet
- Medical EthicsDocument155 pagesMedical EthicsKiran ToorNo ratings yet
- The Pathology of Congestive Heart FailureDocument4 pagesThe Pathology of Congestive Heart FailureMar Ble50% (2)
- Fetal Intervetion - Abdelghaffarhelal2019Document20 pagesFetal Intervetion - Abdelghaffarhelal2019Trần Ngọc BíchNo ratings yet
- Renal QuizDocument2 pagesRenal QuizJune Dumdumaya75% (4)
- Toll Like Receptors Signaling Pathways As A Potential Therapeutic Target in Cardiovascular DiseaseDocument37 pagesToll Like Receptors Signaling Pathways As A Potential Therapeutic Target in Cardiovascular Diseaseeric fantonNo ratings yet
- Gastroenterology by Elagouri MohammedDocument31 pagesGastroenterology by Elagouri MohammedStylesh GuRlyNo ratings yet
- Subjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationDocument18 pagesSubjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationJennalyn Padua SevillaNo ratings yet
- HF DeaDocument53 pagesHF DeaSyifa Mahmud Syukran AkbarNo ratings yet
- Announcement List Displayed Poster 32nd ASMIHADocument36 pagesAnnouncement List Displayed Poster 32nd ASMIHADewi AmeliaNo ratings yet
- Stroke Awareness EducationDocument7 pagesStroke Awareness EducationIneke PutriNo ratings yet
- SympatheticDocument10 pagesSympatheticSharneeshriyaNo ratings yet
- Daftar PustakaDocument6 pagesDaftar Pustakasepty_auliaNo ratings yet