You might also like
- Aub Pogs CPGDocument39 pagesAub Pogs CPGVenz Timothy Wesley LandichoNo ratings yet
- Clinical Guidelines for Diagnosis and Management of DiabetesDocument157 pagesClinical Guidelines for Diagnosis and Management of Diabetesejikieru03100% (3)
- Ob Revalida Review 2017 PDFDocument71 pagesOb Revalida Review 2017 PDFMara Medina - BorleoNo ratings yet
- POGS Clinical Practice Guidelines on Cesarean SectionDocument65 pagesPOGS Clinical Practice Guidelines on Cesarean SectionAngela Caguitla100% (4)
- Digging Up The B0ne BIOCHEMDocument60 pagesDigging Up The B0ne BIOCHEMReina Lyria100% (2)
- Contract To Sell On Land ContractDocument6 pagesContract To Sell On Land ContractKristine-Joy Legaspi FrancoNo ratings yet
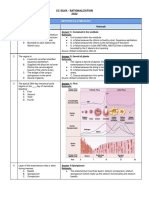
- CC Silva - Rationalization 2022: # Rationale Answer: C. Contained in The Vestibule RationaleDocument34 pagesCC Silva - Rationalization 2022: # Rationale Answer: C. Contained in The Vestibule RationaleNicole Xyza JunsayNo ratings yet
- Hypertension in Pregnancy (Pogs-Cpg)Document55 pagesHypertension in Pregnancy (Pogs-Cpg)Philip Piolo Fuego67% (3)
- OBGYN Revalida Review 2019Document74 pagesOBGYN Revalida Review 2019anonymous100% (1)
- 2022 Pogs Annual Convention SP Rev3 Final - CompressedDocument292 pages2022 Pogs Annual Convention SP Rev3 Final - CompressedKaye HernandezNo ratings yet
- CPG UrogynecologyDocument71 pagesCPG UrogynecologyDjurizzaBustamanteGadin100% (2)
- Managing Diabetes in Pregnancy: A Clinical Practice GuidelineDocument110 pagesManaging Diabetes in Pregnancy: A Clinical Practice GuidelineLisa KriestantoNo ratings yet
- CPG Anemia Pogs 2009Document38 pagesCPG Anemia Pogs 2009Mark Cristopher JoaquinNo ratings yet
- CamScanner document scansDocument166 pagesCamScanner document scansStephy Barluado86% (7)
- Gyne Onco Interns NotesDocument54 pagesGyne Onco Interns NotesCoy NuñezNo ratings yet
- OB - Normal Labor and DeliveryDocument51 pagesOB - Normal Labor and DeliveryJosh Matthew Rosales33% (3)
- (666582801) MKDDocument11 pages(666582801) MKDEdison Tan Santamaria100% (1)
- SGOP cervical cancer guidelinesDocument93 pagesSGOP cervical cancer guidelinesjojolilimomo100% (2)
- Sgop CPG 2008 FinalDocument105 pagesSgop CPG 2008 FinalVia Alip100% (2)
- CPG AbortionDocument40 pagesCPG AbortionKatharine Nerva75% (12)
- CPG-3rd Trimester Bleeding and Postpartum Hemorrage 2009Document107 pagesCPG-3rd Trimester Bleeding and Postpartum Hemorrage 2009lovelots1234100% (8)
- 12 Friedmans Curve v2Document4 pages12 Friedmans Curve v2Jowi Sal100% (1)
- Philippine Obstetrical and Philippine Obstetrical and Gynecological Society (POGS), Foundation, Inc. Gynecological Society (POGS), Foundation, IncDocument51 pagesPhilippine Obstetrical and Philippine Obstetrical and Gynecological Society (POGS), Foundation, Inc. Gynecological Society (POGS), Foundation, IncJanna Janoras ŰNo ratings yet
- Comprehensive Handbook Obstetrics & Gynecology 3rd EdFrom EverandComprehensive Handbook Obstetrics & Gynecology 3rd EdRating: 5 out of 5 stars5/5 (1)
- Understanding the Pathophysiology of PPROMDocument134 pagesUnderstanding the Pathophysiology of PPROMTintalle100% (3)
- Hypertension in Pregnancy (Pogs-Cpg)Document60 pagesHypertension in Pregnancy (Pogs-Cpg)Ivy Combista Baya100% (1)
- CPG-Abnormal Labor and Delivery 2009Document29 pagesCPG-Abnormal Labor and Delivery 2009lovelots123488% (8)
- Ob 1.05 Clinical Practice Guidelines On Immunization For Filipino WomenDocument7 pagesOb 1.05 Clinical Practice Guidelines On Immunization For Filipino Womenotartil_niman50% (2)
- SGOP 2008 (Guidelines On Management)Document87 pagesSGOP 2008 (Guidelines On Management)Via Alip100% (1)
- CPG Preterm Labor PDFDocument90 pagesCPG Preterm Labor PDFJeffrey Arboleda100% (2)
- Nclex-Rn Bullets PondangDocument14 pagesNclex-Rn Bullets PondangKristine-Joy Legaspi FrancoNo ratings yet
- Gynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Document198 pagesGynecology Review: Abigail Elsie Dg. Castro, MD, Maed, Fpogs, Fpsuog August 11, 2017Jojo Mendoza100% (1)
- CPG PSSTDDocument40 pagesCPG PSSTDotartil_niman100% (2)
- Clinical Practice Guidelines For The Obstetrician - GynecologistDocument79 pagesClinical Practice Guidelines For The Obstetrician - GynecologistAngela Caguitla67% (3)
- Introduction To PharmacologyDocument50 pagesIntroduction To PharmacologyAbdishakour Hassa.100% (1)
- OB Gyne ReviewerDocument52 pagesOB Gyne ReviewerRaffy Lucmans100% (1)
- CPG Gestational Trophoblastic DiseasesDocument31 pagesCPG Gestational Trophoblastic DiseasesSMR50% (2)
- MCU-FDT Outpatient ENT ServicesDocument2 pagesMCU-FDT Outpatient ENT ServicesvinbNo ratings yet
- SGOP2019 Cervical Cancer GuidelinesDocument8 pagesSGOP2019 Cervical Cancer GuidelinesNico Angelo CopoNo ratings yet
- CPG Labor and Delivery 2015Document78 pagesCPG Labor and Delivery 2015TintalleNo ratings yet
- Protein Synthesis Inhibitors Classification and MechanismsDocument162 pagesProtein Synthesis Inhibitors Classification and MechanismsCecilia Nguyen100% (1)
- POGS CPG Abnormal Uterine BleedineDocument36 pagesPOGS CPG Abnormal Uterine Bleedinejandale57% (7)
- Gyne - Feu ReviewerDocument87 pagesGyne - Feu ReviewerKoko RoqueNo ratings yet
- Module 6 - Benign Gynecologic TumorsDocument9 pagesModule 6 - Benign Gynecologic TumorsRenz Francis SasaNo ratings yet
- CPG Abortion PDFDocument35 pagesCPG Abortion PDFAlyssaJaneRabayaNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- History and PEDocument3 pagesHistory and PEBom TnaNo ratings yet
- Useful Medications For Oral Conditions: AnalgesicsDocument7 pagesUseful Medications For Oral Conditions: AnalgesicsAswathyNo ratings yet
- TICKLER-PRINT-2 Pedia PDFDocument7 pagesTICKLER-PRINT-2 Pedia PDFCarlos H. AcuñaNo ratings yet
- CPG On Hypertension in PregnancyDocument91 pagesCPG On Hypertension in PregnancyRumelle Reyes100% (3)
- Clinical Guidelines for Safe ChildbirthDocument52 pagesClinical Guidelines for Safe Childbirthdennisreveni100% (1)
- Planes and Diameters of The PelvisDocument32 pagesPlanes and Diameters of The PelvisRumelle ReyesNo ratings yet
- Two Up Cont CPG Intrapartum PDFDocument98 pagesTwo Up Cont CPG Intrapartum PDFjojolilimomoNo ratings yet
- Finals QuestionsDocument10 pagesFinals QuestionsBobet ReñaNo ratings yet
- Digging Up The Bones - MicrobiologyDocument31 pagesDigging Up The Bones - MicrobiologyMossa Di Base100% (1)
- Diagnosis and Management of Gestational Trophoblastic Disease C rat w o ie M ev S R G PODocument56 pagesDiagnosis and Management of Gestational Trophoblastic Disease C rat w o ie M ev S R G PORendy Adhitya PratamaNo ratings yet
- OB 1.01 DystociaDocument9 pagesOB 1.01 DystociaRaquel Reyes100% (1)
- Pediatric Tickler by RemDocument7 pagesPediatric Tickler by RemRem AlfelorNo ratings yet
- Clincal Practice Guidelines For Diabetes in The PhilippinesDocument40 pagesClincal Practice Guidelines For Diabetes in The PhilippinesRans NosceNo ratings yet
- Diabetes Mellitus CPGDocument137 pagesDiabetes Mellitus CPGKristine-Joy Legaspi FrancoNo ratings yet
- Endocrine Dr. RehabDocument65 pagesEndocrine Dr. RehabMohammed Saad NabhanNo ratings yet
- Update On: Diabetes MellitusDocument37 pagesUpdate On: Diabetes MellitusDr. Mamunul Abedin100% (1)
- Diabetes: Amjad Al ShdaifatDocument94 pagesDiabetes: Amjad Al ShdaifatRand AhmadNo ratings yet
- Diagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Document48 pagesDiagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Carolina González RiveraNo ratings yet
- Konsensus DM Ada Esda & PerkeniDocument31 pagesKonsensus DM Ada Esda & PerkeniWindy SuryaNo ratings yet
- Diabetes Mellitus CPGDocument137 pagesDiabetes Mellitus CPGKristine-Joy Legaspi FrancoNo ratings yet
- Clinical History of 1yo Female with PneumoniaDocument4 pagesClinical History of 1yo Female with PneumoniaKristine-Joy Legaspi FrancoNo ratings yet
- FMCH History No. 2Document4 pagesFMCH History No. 2Kristine-Joy Legaspi FrancoNo ratings yet
- Case Report on 53yo Female with Numbness and DiabetesDocument7 pagesCase Report on 53yo Female with Numbness and DiabetesKristine-Joy Legaspi FrancoNo ratings yet
- Cuidados Diabetes 2016Document119 pagesCuidados Diabetes 2016Diego Pizarro ReyesNo ratings yet
- Community-Acquired Pneumonia GuideDocument37 pagesCommunity-Acquired Pneumonia GuideKristine-Joy Legaspi FrancoNo ratings yet
- ANTIviralDocument9 pagesANTIviralKristine-Joy Legaspi FrancoNo ratings yet
- 1diabetes United For Diabetes PhilDocument20 pages1diabetes United For Diabetes PhilKristine-Joy Legaspi FrancoNo ratings yet
- 2016 Ndep Adas Standards of Medical Care in DiabetesDocument54 pages2016 Ndep Adas Standards of Medical Care in DiabetesKristine-Joy Legaspi FrancoNo ratings yet
- Ampicillin Nursing ConsiderationsDocument5 pagesAmpicillin Nursing ConsiderationsKristine-Joy Legaspi FrancoNo ratings yet
- BCG Vaccine: Tuberculosis, The Variable Effectiveness of The Vaccine Against Adult Pulmonary TB, and The Vaccine'sDocument10 pagesBCG Vaccine: Tuberculosis, The Variable Effectiveness of The Vaccine Against Adult Pulmonary TB, and The Vaccine'sKristine-Joy Legaspi FrancoNo ratings yet
- Anti DMDocument9 pagesAnti DMKristine-Joy Legaspi FrancoNo ratings yet
- NCPs AgeDocument5 pagesNCPs AgeKristine-Joy Legaspi FrancoNo ratings yet
- GastrointestinalDocument2 pagesGastrointestinalKristine-Joy Legaspi FrancoNo ratings yet
- Fentanyl Citrate Injection, USP: RX Only DescriptionDocument7 pagesFentanyl Citrate Injection, USP: RX Only DescriptionWidy WidyNo ratings yet
- Label ObatDocument24 pagesLabel Obateruga9No ratings yet
- Previous Year Board Exam Questions (2007-2016) : Chemistry in Everyday LifeDocument6 pagesPrevious Year Board Exam Questions (2007-2016) : Chemistry in Everyday Lifehoney1002No ratings yet
- Drug StudyDocument9 pagesDrug StudyAysaaa DCNo ratings yet
- Study ScheduleDocument3 pagesStudy ScheduleMan DipNo ratings yet
- Marketing Mix Concept Based On One Pharmaceutical Company ProductDocument12 pagesMarketing Mix Concept Based On One Pharmaceutical Company ProductDlow LopSkfnNo ratings yet
- Pharmaceutical Formulations III Pharm DQuestion BankDocument7 pagesPharmaceutical Formulations III Pharm DQuestion BankAnanda VijayasarathyNo ratings yet
- PKPD For BeginnersDocument31 pagesPKPD For Beginnerstanty_ukNo ratings yet
- Aroosa Qamar PharmacologyDocument17 pagesAroosa Qamar PharmacologyAdan IsrarNo ratings yet
- Dexamethasone PAR SummaryDocument17 pagesDexamethasone PAR SummaryJagdish ChanderNo ratings yet
- The Four Phases of Clinical Trials - June 2016 1Document1 pageThe Four Phases of Clinical Trials - June 2016 1Mihir OzaNo ratings yet
- Anexos Finales 5 - 6 - 7 - 8 - 9Document403 pagesAnexos Finales 5 - 6 - 7 - 8 - 9Mile Castillo VillarealNo ratings yet
- Alkylating AgentsDocument3 pagesAlkylating AgentsJonathan ObañaNo ratings yet
- Amiodarone IV Administration 1.0Document5 pagesAmiodarone IV Administration 1.0Ari BinkosimNo ratings yet
- Body Surface Area Body Surface AreaDocument4 pagesBody Surface Area Body Surface AreaJose Hady PuteraNo ratings yet
- AnalgesicDocument47 pagesAnalgesicMOHAMAD ZULFIKRIE ABASNo ratings yet
- Imci Drug StudyDocument4 pagesImci Drug StudyDea Sabelle CastroNo ratings yet
- Dosage CalculationsDocument8 pagesDosage CalculationsReinna Angel CampoNo ratings yet
- ER Clinical NotesDocument23 pagesER Clinical NotesmngaNo ratings yet
- Total Estradiol LectureDocument68 pagesTotal Estradiol LectureLucas ElyNo ratings yet
- ANTIBIOTICS (抗生素製劑) : Md300500 Application Manual Of Medicines (藥品使用摘要) Rev.22 / DEC. 2021Document11 pagesANTIBIOTICS (抗生素製劑) : Md300500 Application Manual Of Medicines (藥品使用摘要) Rev.22 / DEC. 2021Linh PhạmNo ratings yet
- Commonly Used Chemotherapy Drugs: MedicationsDocument6 pagesCommonly Used Chemotherapy Drugs: MedicationsAndra Elena PricopNo ratings yet
- Project MBA Ranbaxy Laboratories Ltd.Document5 pagesProject MBA Ranbaxy Laboratories Ltd.neelamverma1970No ratings yet
- Basetext SingleDocument129 pagesBasetext SingleJiHyun ParkNo ratings yet
- PD3 - Dose-Response Relationship - Akm-050116 PDFDocument27 pagesPD3 - Dose-Response Relationship - Akm-050116 PDFSindhu Babu100% (1)
- Farmakologi KlinikDocument21 pagesFarmakologi KlinikagniajolandaNo ratings yet
- Salofalk Tablets PI 1220Document13 pagesSalofalk Tablets PI 1220Geo GeoNo ratings yet