You might also like
- Entitlement Cure SampleDocument34 pagesEntitlement Cure SampleZondervan100% (1)
- Muscles of MasticationDocument27 pagesMuscles of MasticationNanditha Swaroop100% (2)
- Textbook Of: Ear, Nose, Throat SurgeryDocument23 pagesTextbook Of: Ear, Nose, Throat SurgeryOliver Scissors100% (1)
- BD Chaurasia's Human Anatomy - 2017 - Head & Neck, Volume 3, CBS Publishers, 7th Edition 2017-TLS PDFDocument344 pagesBD Chaurasia's Human Anatomy - 2017 - Head & Neck, Volume 3, CBS Publishers, 7th Edition 2017-TLS PDFAndrei Tutu85% (13)
- 6.nerves of Head and NeckDocument36 pages6.nerves of Head and NeckDr P N N ReddyNo ratings yet
- CEMENTUMDocument50 pagesCEMENTUMDENTALORG.COM100% (1)
- Facial NerveDocument87 pagesFacial NerveKishor BhandariNo ratings yet
- Maji - Josh .Dental-Book PDFDocument614 pagesMaji - Josh .Dental-Book PDFMohammed hisham khan92% (13)
- Anatomy of The Facial NerveDocument75 pagesAnatomy of The Facial NerveSerene Batra100% (2)
- Facial NerveDocument80 pagesFacial Nerverasagna reddyNo ratings yet
- Seminar On Radicular CystDocument7 pagesSeminar On Radicular CystKhalid Mahmud Arifin100% (2)
- Anterior Triangle of The Neck JDVDocument5 pagesAnterior Triangle of The Neck JDVNica Lopez Fernandez100% (3)
- Anatomy of Facial Nerve New PDFDocument37 pagesAnatomy of Facial Nerve New PDFDeepak Kumar100% (1)
- Parotid GlandDocument24 pagesParotid GlandkeerthanaNo ratings yet
- Dri InternshipDocument38 pagesDri InternshipGuruprasad Sanga100% (3)
- Facial Nerve and Its Applied AnatomyDocument37 pagesFacial Nerve and Its Applied Anatomyherojittlc100% (1)
- 20.short Notes and Short Cases in ENT PDFDocument116 pages20.short Notes and Short Cases in ENT PDFpakistan100% (1)
- ENT Head and Neck ExamDocument21 pagesENT Head and Neck ExamvickyNo ratings yet
- Healing of Extraction SocketDocument34 pagesHealing of Extraction SocketIndrani Das93% (14)
- Dept ENT PDFDocument117 pagesDept ENT PDFPravee GaddeNo ratings yet
- Head and NeckDocument11 pagesHead and NeckHisham ChomanyNo ratings yet
- "Next Friend" and "Guardian Ad Litem" - Difference BetweenDocument1 page"Next Friend" and "Guardian Ad Litem" - Difference BetweenTeh Hong Xhe100% (2)
- Pharmacology Record For BDS As Per KUHSDocument44 pagesPharmacology Record For BDS As Per KUHSthomasarun2009100% (1)
- Surgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDocument32 pagesSurgical Anatomy of Parotid Gland - Ommos - Edition-01-SoiDr Prashant Kumar100% (1)
- Emergency Cardiology 2E PDFDocument289 pagesEmergency Cardiology 2E PDFRao Rizwan ShakoorNo ratings yet
- Deviated Nasal SeptumDocument20 pagesDeviated Nasal SeptummalathiNo ratings yet
- Method Statement (RC Slab)Document3 pagesMethod Statement (RC Slab)group2sd131486% (7)
- Kazi Guide Mbbs AnatomyDocument5 pagesKazi Guide Mbbs Anatomychandan50% (10)
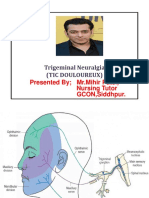
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- Muscles of MasticationDocument75 pagesMuscles of Masticationbhasalepooja100% (1)
- Anand's Human Anatomy For Dental Students, 3rd EditionDocument762 pagesAnand's Human Anatomy For Dental Students, 3rd Editionviaerea100% (4)
- Cranial Nerve AssessmentDocument42 pagesCranial Nerve AssessmentValeryn Quiman100% (7)
- Head InjuryDocument31 pagesHead InjuryZawawi Ibnu Rosyid0% (1)
- SUPPORTS OF UTERUS ShilpaDocument61 pagesSUPPORTS OF UTERUS ShilpaSreelasya83% (6)
- Bacterial Genome Assembly IlluminaDocument49 pagesBacterial Genome Assembly IlluminadksaNo ratings yet
- Facial Nerve MCQDocument4 pagesFacial Nerve MCQIqbal Syed100% (1)
- Ear ExaminationDocument47 pagesEar ExaminationHarshit Bhardwaj100% (4)
- Manipal Manual of Clinical Medicine by B. A. Shastry: Read Online and Download EbookDocument6 pagesManipal Manual of Clinical Medicine by B. A. Shastry: Read Online and Download EbookVignesh Jaya88% (8)
- Neha ShahDocument448 pagesNeha ShahAnkita Rana100% (3)
- Republic Act No. 10389Document5 pagesRepublic Act No. 10389Marge RoseteNo ratings yet
- Facial NerveDocument128 pagesFacial NervevaneetNo ratings yet
- CSF RhinorrheaDocument10 pagesCSF RhinorrheaDr-Firas Nayf Al-ThawabiaNo ratings yet
- Shafer S Textbook of Oral PathologyDocument6 pagesShafer S Textbook of Oral PathologyAbhishek Chauhan0% (2)
- Salivary GlandsDocument68 pagesSalivary GlandsTatiana Decuseară100% (1)
- Ananth Narayan and Paniker 11th EditionDocument42 pagesAnanth Narayan and Paniker 11th EditionArjun Kandara50% (2)
- Oral Pathology - Physical & Chemical Injuries of Oral CavityDocument44 pagesOral Pathology - Physical & Chemical Injuries of Oral CavityRachit Srivastava83% (18)
- Life Cycle of AmeloblastDocument14 pagesLife Cycle of Ameloblastimi486% (7)
- Impact of Employee Motivation in The Banking SectorDocument48 pagesImpact of Employee Motivation in The Banking Sectormohd talalNo ratings yet
- Medical Surgical Nursing:Ear, Nose, and Throat Disorder.Document126 pagesMedical Surgical Nursing:Ear, Nose, and Throat Disorder.Minlik-alew Dejenie89% (18)
- Physiotherapy Practice Guidelines For COPDDocument35 pagesPhysiotherapy Practice Guidelines For COPD健康生活園Healthy Life Garden100% (1)
- Anatomy of Facial NerveDocument46 pagesAnatomy of Facial NerveAvinash SitaramanNo ratings yet
- Chest Wall DeformitiesDocument25 pagesChest Wall DeformitiesRaghu NadhNo ratings yet
- The Ear. The Helix. The External Auditory Canal and Tympanic Membrane. Air and Bone JoiningDocument40 pagesThe Ear. The Helix. The External Auditory Canal and Tympanic Membrane. Air and Bone JoiningHarshit BhardwajNo ratings yet
- DAILY ROUND Head NurseDocument1 pageDAILY ROUND Head NurseRao Rizwan ShakoorNo ratings yet
- Ectropion vs. EntropionDocument1 pageEctropion vs. EntropionAhmed ShafikNo ratings yet
- Health Promotion Officers - CPD Booklet Schedule PDFDocument5 pagesHealth Promotion Officers - CPD Booklet Schedule PDFcharles KadzongaukamaNo ratings yet
- Bronchial AsthmaDocument27 pagesBronchial AsthmaRenuka Sivaram100% (4)
- Carcinoma TongueDocument39 pagesCarcinoma TongueVijay Krishna Murthy33% (3)
- Learning Objective: at The End of The Exercise Students Shall Be Able ToDocument3 pagesLearning Objective: at The End of The Exercise Students Shall Be Able ToAni Gupta100% (1)
- Physiology of PainDocument23 pagesPhysiology of PainSarad Chand Yadav100% (1)
- Inflammation. Etiology. Vascular Changes. Cellular Events in Inflammation. Acute Inflammation. Morphologic PatternsDocument57 pagesInflammation. Etiology. Vascular Changes. Cellular Events in Inflammation. Acute Inflammation. Morphologic PatternsZauzaNo ratings yet
- CherubismDocument12 pagesCherubismSureeratPatima100% (1)
- Deviated Nasal SeptumDocument15 pagesDeviated Nasal SeptumSrinivas Sukhavasi50% (2)
- Practical PerformaDocument4 pagesPractical PerformaVijay Pradeep100% (3)
- Omr Case HistoryDocument39 pagesOmr Case HistoryAnuMPaul0% (1)
- TympanoplastyDocument34 pagesTympanoplastymanu100% (1)
- Lec 3 Range of Muscle WorkDocument16 pagesLec 3 Range of Muscle Worksajeel100% (1)
- Dural Venous SinusesDocument31 pagesDural Venous Sinusesveegeer100% (1)
- Physiology PDFDocument98 pagesPhysiology PDFSARJIL AMIN67% (3)
- Facial Nerve 2Document87 pagesFacial Nerve 2bhavyaNo ratings yet
- Cranial NervesDocument7 pagesCranial NerveshamnahrjunaidNo ratings yet
- Nebulisation Chart: Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7Document1 pageNebulisation Chart: Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7Rao Rizwan ShakoorNo ratings yet
- Knee HeightDocument1 pageKnee HeightRao Rizwan ShakoorNo ratings yet
- Financial Details: Individual Claim FormDocument1 pageFinancial Details: Individual Claim FormRao Rizwan ShakoorNo ratings yet
- Medical Certificat1Document1 pageMedical Certificat1Rao Rizwan ShakoorNo ratings yet
- Upper Gi Endoscopy ReportDocument2 pagesUpper Gi Endoscopy ReportRao Rizwan ShakoorNo ratings yet
- DISCHARGEDocument1 pageDISCHARGERao Rizwan ShakoorNo ratings yet
- Round NotesDocument1 pageRound NotesRao Rizwan ShakoorNo ratings yet
- Bts Guideline For Oxygen Use in Adults in Healthcare and Emergency SettingsDocument100 pagesBts Guideline For Oxygen Use in Adults in Healthcare and Emergency SettingsalbarkatNo ratings yet
- Complete Entry DataDocument28 pagesComplete Entry DataRao Rizwan ShakoorNo ratings yet
- Round Note1... A4Document1 pageRound Note1... A4Rao Rizwan ShakoorNo ratings yet
- ACR-NPF Psoriatic Arthritis Guideline Project PlanDocument20 pagesACR-NPF Psoriatic Arthritis Guideline Project PlanalbarkatNo ratings yet
- Jcem 0709Document20 pagesJcem 0709Rao Rizwan ShakoorNo ratings yet
- Income TaxDocument1 pageIncome TaxRao Rizwan ShakoorNo ratings yet
- Jcem 0709Document20 pagesJcem 0709Rao Rizwan ShakoorNo ratings yet
- Jiqr": Ar, R,?TT TLLDocument1 pageJiqr": Ar, R,?TT TLLRao Rizwan ShakoorNo ratings yet
- Common Medical Abbreviations: SUB Script SubscriptDocument10 pagesCommon Medical Abbreviations: SUB Script SubscriptYing Jie LiowNo ratings yet
- Jcem 4227Document23 pagesJcem 4227Rao Rizwan ShakoorNo ratings yet
- Turgor KulitDocument21 pagesTurgor KulitChairunisa AnggrainiNo ratings yet
- NHSSB Wound Management ManualDocument102 pagesNHSSB Wound Management ManualxcalibursysNo ratings yet
- Diagnosis Management Hepatic EncephalopathyDocument21 pagesDiagnosis Management Hepatic EncephalopathyRao Rizwan ShakoorNo ratings yet
- Hepaticencephenhanced PDFDocument74 pagesHepaticencephenhanced PDFRao Rizwan ShakoorNo ratings yet
- Methodological Considerations When Using Non-Invasive Tests: General StatementsDocument1 pageMethodological Considerations When Using Non-Invasive Tests: General StatementsRao Rizwan ShakoorNo ratings yet
- Common Medical Abbreviations: SUB Script SubscriptDocument10 pagesCommon Medical Abbreviations: SUB Script SubscriptYing Jie LiowNo ratings yet
- Recording of Fluid Balance Intake-Output PolicyDocument7 pagesRecording of Fluid Balance Intake-Output PolicyRao Rizwan ShakoorNo ratings yet
- Medical Symbols List2Document1 pageMedical Symbols List2Rao Rizwan ShakoorNo ratings yet
- PatientLeavefromAcuteInpatientUnitPolicy v4 Mar2012Document10 pagesPatientLeavefromAcuteInpatientUnitPolicy v4 Mar2012Rao Rizwan ShakoorNo ratings yet
- Tab 6 F Guidelines For Death PronouncementDocument2 pagesTab 6 F Guidelines For Death PronouncementRao Rizwan ShakoorNo ratings yet
- Join Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsDocument24 pagesJoin Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsNaveen KumarNo ratings yet
- PEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesDocument2 pagesPEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesLady Diana TiangcoNo ratings yet
- Task 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Document5 pagesTask 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Samir Mosquera-PalominoNo ratings yet
- Cultivation Vaderstad Manual 2017Document128 pagesCultivation Vaderstad Manual 2017deroryNo ratings yet
- Sop For Enlistment of Engineering ConsultantsDocument1 pageSop For Enlistment of Engineering Consultantssatheb319429No ratings yet
- Study Notes On Isomers and Alkyl HalidesDocument3 pagesStudy Notes On Isomers and Alkyl HalidesChristian Josef AvelinoNo ratings yet
- 3 Activities For Adults To Practice Modeling SELDocument10 pages3 Activities For Adults To Practice Modeling SELDavid Garcia PerezNo ratings yet
- ALL102-Walker Shirley-Unemployed at Last-The Monkeys Mask and The Poetics of Excision-Pp72-85Document15 pagesALL102-Walker Shirley-Unemployed at Last-The Monkeys Mask and The Poetics of Excision-Pp72-85PNo ratings yet
- Epo-Fix Plus: High-Performance Epoxy Chemical AnchorDocument3 pagesEpo-Fix Plus: High-Performance Epoxy Chemical Anchormilivoj ilibasicNo ratings yet
- Anti Stain Nsl30 Super - Msds - SdsDocument8 pagesAnti Stain Nsl30 Super - Msds - SdsS.A. MohsinNo ratings yet
- Discharge PlanDocument3 pagesDischarge PlanBALOGO TRISHA MARIENo ratings yet
- Guides To The Freshwater Invertebrates of Southern Africa Volume 2 - Crustacea IDocument136 pagesGuides To The Freshwater Invertebrates of Southern Africa Volume 2 - Crustacea IdaggaboomNo ratings yet
- Revision Ror The First TermDocument29 pagesRevision Ror The First TermNguyễn MinhNo ratings yet
- 2019 06 28 PDFDocument47 pages2019 06 28 PDFTes BabasaNo ratings yet
- Comprehensive Safe Hospital FrameworkDocument12 pagesComprehensive Safe Hospital FrameworkEbby OktaviaNo ratings yet
- Installing Touareg R5 CamshaftDocument1 pageInstalling Touareg R5 CamshaftSarunas JurciukonisNo ratings yet
- Leather & Polymer - Lec01.2k11Document11 pagesLeather & Polymer - Lec01.2k11Anik AlamNo ratings yet
- 6Document2 pages6Min Hsuan HsianNo ratings yet
- How McDonald'sDocument2 pagesHow McDonald'spratik khandualNo ratings yet
- Maintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBDocument10 pagesMaintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBAtaa AssaadNo ratings yet
- WWW Spectrosci Com Product Infracal Model CVH PrinterFriendlDocument3 pagesWWW Spectrosci Com Product Infracal Model CVH PrinterFriendlather1985No ratings yet
- Feeder BrochureDocument12 pagesFeeder BrochureThupten Gedun Kelvin OngNo ratings yet