You might also like
- Project Report Multispeciality HospitalDocument13 pagesProject Report Multispeciality HospitalChetan Kabra87% (15)
- Criticare 8100 Owners Manual PDFDocument182 pagesCriticare 8100 Owners Manual PDFKroumson Ben AboubacarNo ratings yet
- Physiology of PregnancyDocument31 pagesPhysiology of PregnancyPutra Mahautama100% (1)
- PBL SS 2 - Fetal DevelopmentDocument3 pagesPBL SS 2 - Fetal DevelopmentJellie MendozaNo ratings yet
- Upper Limb - Pectoral Region, Scapular Region, Axilla & Brachial PlexusDocument12 pagesUpper Limb - Pectoral Region, Scapular Region, Axilla & Brachial Plexusewijayapala100% (1)
- My Pediatric Rotation ReflectionsDocument4 pagesMy Pediatric Rotation ReflectionsAdepoju Victor AbiolaNo ratings yet
- Final 1 - Mankind Pharma ReportDocument133 pagesFinal 1 - Mankind Pharma ReportMahabalaNo ratings yet
- Development of GITDocument88 pagesDevelopment of GITBindiya MangarNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Lecture 9 The Digestive SystemDocument59 pagesLecture 9 The Digestive SystemMatthew Bargo100% (2)
- Body CavitiesDocument22 pagesBody Cavitiesapi-421876727100% (1)
- Tissue - SeeleyDocument61 pagesTissue - SeeleyJuli Damayanty Harahap100% (1)
- EthicsDocument77 pagesEthicsAce Visuals100% (2)
- Visual SystemDocument6 pagesVisual SystemJobelle Acena100% (1)
- Histology of Male Reproductive SystemDocument56 pagesHistology of Male Reproductive SystemMuhammad Irfan100% (2)
- Lecture 2-Blood RBC WBCDocument51 pagesLecture 2-Blood RBC WBCsamayaNo ratings yet
- Fluid and Electrolyte Management of The Surgical PatientDocument26 pagesFluid and Electrolyte Management of The Surgical PatientYudhi Leo PrimaNo ratings yet
- Chapter 3Document96 pagesChapter 3Sinclyr Valenciano100% (2)
- Family Abuse and NeglectDocument20 pagesFamily Abuse and Neglectapi-311788459100% (1)
- Community MedicineDocument248 pagesCommunity MedicineFaisal MahbubNo ratings yet
- Female ReproductiveDocument34 pagesFemale ReproductiveAbdallah A. Abu Mattar100% (2)
- WHO Action - Plan DisabilityDocument28 pagesWHO Action - Plan DisabilityJosé Queiroz100% (1)
- Introduction To The Gastrointestinal SystemDocument10 pagesIntroduction To The Gastrointestinal Systemjaninesimbol24No ratings yet
- Respiratorysystem 120105050542 Phpapp01Document43 pagesRespiratorysystem 120105050542 Phpapp01Buuvee BeNo ratings yet
- 4 19 Lymphmatic SystemDocument10 pages4 19 Lymphmatic SystemJohn Lawrence Ybanez100% (1)
- 1 Introduction To The Gastrointestinal SystemDocument7 pages1 Introduction To The Gastrointestinal SystemLinh Phan100% (1)
- Clinical Anatomy of The Esophagus and StomachDocument82 pagesClinical Anatomy of The Esophagus and StomachmackieccNo ratings yet
- Histology of Git and Circulatory SystemDocument45 pagesHistology of Git and Circulatory SystemRan CelNo ratings yet
- H 4.2 Histology Urinary SystemDocument52 pagesH 4.2 Histology Urinary SystemF N100% (2)
- Eye AnatomyDocument21 pagesEye AnatomyHammad afzal100% (2)
- Respiratory SystemDocument6 pagesRespiratory Systemjenryl100% (1)
- Histology of Glands: Dr. Zana TahseenDocument28 pagesHistology of Glands: Dr. Zana TahseenAhmed JawdetNo ratings yet
- Embryology Reviewer Chapter 1 and 2Document9 pagesEmbryology Reviewer Chapter 1 and 2Allison Eunice ServandoNo ratings yet
- Cell-Structure and FunctionDocument15 pagesCell-Structure and FunctionNILKAMAL CHAUDHARYNo ratings yet
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahNo ratings yet
- Fetal DevelopmentDocument4 pagesFetal DevelopmentAnonymous bq4KY0mcWGNo ratings yet
- Accessory OrgansDocument18 pagesAccessory OrgansDaniel AtiehNo ratings yet
- Anatomy of The Eye PDFDocument15 pagesAnatomy of The Eye PDFPaolo Naguit0% (1)
- Anatomy and Physiology Case PresentationDocument3 pagesAnatomy and Physiology Case PresentationVito VitoNo ratings yet
- Diagnostic Procedures of PregnancyDocument7 pagesDiagnostic Procedures of PregnancyRuth Anne Zonio DamasoNo ratings yet
- MenstruationDocument16 pagesMenstruationAnnsha VeimernNo ratings yet
- PregnancyDocument31 pagesPregnancyAnonymous Yqk1j9ANo ratings yet
- Non - Infectiouse Disease Prevention and controlfINALDocument80 pagesNon - Infectiouse Disease Prevention and controlfINALbiniam yohannesNo ratings yet
- Histology of The Special SenseDocument84 pagesHistology of The Special SenseRushda100% (1)
- CPC-Patho Version 6Document20 pagesCPC-Patho Version 6Bea SamonteNo ratings yet
- Intrdoduction Gis 2 (Associated Organs) : Maya Tejasari Histology DepartmentDocument24 pagesIntrdoduction Gis 2 (Associated Organs) : Maya Tejasari Histology DepartmentIpan YustiartaNo ratings yet
- The Muscular SystemDocument183 pagesThe Muscular SystemRochelle Antig100% (2)
- Anatomy & Physiology Outlines - Finals (Chapter 16: Digestive)Document15 pagesAnatomy & Physiology Outlines - Finals (Chapter 16: Digestive)Dahrell Lopez BautistaNo ratings yet
- DIgestion and Absorption of CarbohydratesDocument35 pagesDIgestion and Absorption of CarbohydratesAtif Amin Baig100% (1)
- Embryology of Urogenital SystemDocument42 pagesEmbryology of Urogenital SystemAngetile Kasanga100% (1)
- VitaminsDocument68 pagesVitaminsalthea vergaraNo ratings yet
- Tubal LigationDocument14 pagesTubal LigationGrace Ann DacuanNo ratings yet
- GastrointestinalDocument39 pagesGastrointestinalالمسوول الاعلاميNo ratings yet
- K2 - Histology of Cardiovascular SystemDocument88 pagesK2 - Histology of Cardiovascular SystemAyustiaFaniF100% (1)
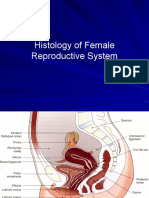
- Histology of Female Reproductive System 2020Document45 pagesHistology of Female Reproductive System 2020Devina Kriskineya100% (2)
- Anatomy of The EyesDocument35 pagesAnatomy of The EyesKiela Nicole Gatpandan AguilarNo ratings yet
- Gynecological Anatomy & PhysiologyDocument39 pagesGynecological Anatomy & Physiologynursereview100% (3)
- Shock: Blood TransfusionDocument81 pagesShock: Blood TransfusionBir Mohammad SonetNo ratings yet
- Histology of The Digestive SystemDocument46 pagesHistology of The Digestive SystemM Reza Rizqi INo ratings yet
- Fetal DevelopmentDocument15 pagesFetal DevelopmentOmar HammadNo ratings yet
- Fertilization and Fetal Development Abd CirculiationDocument54 pagesFertilization and Fetal Development Abd CirculiationMohnnad Hmood AlgaraybhNo ratings yet
- Lymphatic SystemDocument29 pagesLymphatic SystemlecturioNo ratings yet
- Lymph SystemDocument7 pagesLymph SystemghaiathNo ratings yet
- The Human Body A Nutrition PerspectiveDocument50 pagesThe Human Body A Nutrition PerspectiveRichard GelmanNo ratings yet
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaNo ratings yet
- Prevalance BipolarDocument11 pagesPrevalance BipolarrifkaraihanaNo ratings yet
- Cannabis and BehaviorDocument10 pagesCannabis and BehaviorPRMurphyNo ratings yet
- Link TTG GoutDocument1 pageLink TTG GoutrifkaraihanaNo ratings yet
- Skripsi. Jurnal Untan - Ac.id Miopi PDFDocument20 pagesSkripsi. Jurnal Untan - Ac.id Miopi PDFrifkaraihanaNo ratings yet
- Tranexamic Acid For Spontaneous Intracerebral Hemorrhage A Randomized Controlled Pilot TrialDocument7 pagesTranexamic Acid For Spontaneous Intracerebral Hemorrhage A Randomized Controlled Pilot TrialAnsh NviariyntiNo ratings yet
- Association Between Hemorrhagic Stroke Occurrence and Meteorological Factors and PollutantsDocument8 pagesAssociation Between Hemorrhagic Stroke Occurrence and Meteorological Factors and PollutantsrifkaraihanaNo ratings yet
- Cerebritis & Abses OtakDocument17 pagesCerebritis & Abses OtakrifkaraihanaNo ratings yet
- Jonathan Edlow, Magdy Selim Neurology Emergencies 2010Document251 pagesJonathan Edlow, Magdy Selim Neurology Emergencies 2010Alina AndreiNo ratings yet
- 4-Lens and CataractDocument59 pages4-Lens and CataractSa'adah Munawaroh HDNo ratings yet
- 4 RetinaDocument59 pages4 RetinajanechaterineNo ratings yet
- Head Injury NICE GuidelineDocument54 pagesHead Injury NICE GuidelineIrina Garlea-RobuNo ratings yet
- Head InjuryDocument61 pagesHead InjuryRicky Cornelius TariganNo ratings yet
- Low Birthweight From EYDocument31 pagesLow Birthweight From EYDhara IkjNo ratings yet
- Pediatric Abx Surg Proph GuidelineDocument2 pagesPediatric Abx Surg Proph GuidelinerifkaraihanaNo ratings yet
- HomeopathyDocument18 pagesHomeopathypksharma75No ratings yet
- Placenta PreviaDocument8 pagesPlacenta PreviaBj DuquesaNo ratings yet
- Resource ListDocument5 pagesResource Listapi-405635445No ratings yet
- Precedex Dosing GuidelinesDocument15 pagesPrecedex Dosing GuidelinesemonhalimNo ratings yet
- Op-Trop200130 1..11Document11 pagesOp-Trop200130 1..11Desianus Salmon WaaNo ratings yet
- Diabetic KetoacidosisDocument7 pagesDiabetic KetoacidosisetengNo ratings yet
- Late Lower Incisor CrowdingDocument18 pagesLate Lower Incisor CrowdingHaffie HafiziNo ratings yet
- 1 The Philippines Sam Guidelines 2015 Final Print Ready PDFDocument111 pages1 The Philippines Sam Guidelines 2015 Final Print Ready PDFFar SultanNo ratings yet
- Paediatric OtorhinolaryngologyDocument37 pagesPaediatric OtorhinolaryngologySana BushraNo ratings yet
- Piis1073874613000777 PDFDocument20 pagesPiis1073874613000777 PDFdrzana78No ratings yet
- Comparative Study of Epidural Fentanyl and Buprenorphine For Post Operative Analgesia in Lower Abdominal and Lower Limb SurgeriesDocument8 pagesComparative Study of Epidural Fentanyl and Buprenorphine For Post Operative Analgesia in Lower Abdominal and Lower Limb SurgeriesIOSRjournalNo ratings yet
- Complete Denture Occlusion PDFDocument25 pagesComplete Denture Occlusion PDFÄpriolia SuNo ratings yet
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 pagesPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamNo ratings yet
- Catalase Test - Principle, Procedure and Interpretations - HowMedDocument3 pagesCatalase Test - Principle, Procedure and Interpretations - HowMedMeenachi ChidambaramNo ratings yet
- Zirconnia Knife Edge PDFDocument6 pagesZirconnia Knife Edge PDFMuaiyed Buzayan AkremyNo ratings yet
- Dengue Nov2019Document87 pagesDengue Nov2019Marie Razel Lopez100% (1)
- Neurology, Neurosurgery MCQ PointsDocument32 pagesNeurology, Neurosurgery MCQ PointsBruno86% (7)
- Down SyndromeDocument74 pagesDown Syndromeanumeha sharma100% (2)
- Dental School Personal StatementDocument1 pageDental School Personal StatementOboeadam912No ratings yet
- Makalah Bahasa InggrisDocument11 pagesMakalah Bahasa Inggrismei diana sara'isNo ratings yet
- Forearm and Wrist FracturesDocument34 pagesForearm and Wrist FracturesFatemeh DerakhshanNo ratings yet
- Foundations of Special Education, Michael FarrelDocument11 pagesFoundations of Special Education, Michael FarrelHugo SáNo ratings yet
- Review of Orthopaedic Trauma 2e 2013 PDF Unitedvrg PDFDocument568 pagesReview of Orthopaedic Trauma 2e 2013 PDF Unitedvrg PDFWahyu Alamsyah DasopangNo ratings yet
- ASIA WorksheetDocument2 pagesASIA WorksheetDinar Yudistira FirdausNo ratings yet
- 10-037.16 Medical Emergency ProceduresDocument2 pages10-037.16 Medical Emergency Proceduressuperm0mof6No ratings yet
- Eng - PB 2016 FinalDocument6 pagesEng - PB 2016 Finalashok PradhanNo ratings yet