You might also like
- DOC571RevC AesculapNeedleComparisonChart 3 FoldBrochureDocument2 pagesDOC571RevC AesculapNeedleComparisonChart 3 FoldBrochureMuhammad SaadNo ratings yet
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadNo ratings yet
- Residency Survival Guide: Canadian Association of General Surgeons Residents CommitteeDocument53 pagesResidency Survival Guide: Canadian Association of General Surgeons Residents CommitteeIrina MincuNo ratings yet
- IndexDocument2 pagesIndexMuhammad SaadNo ratings yet
- SurgeryDocument6 pagesSurgeryMuhammad Saad100% (1)
- Therapeutic EnzymesDocument39 pagesTherapeutic EnzymesMuhammad SaadNo ratings yet
- Guidelines For: Continuing Medical Education (CME) / Continuing Dental Education (eDE)Document12 pagesGuidelines For: Continuing Medical Education (CME) / Continuing Dental Education (eDE)Muhammad SaadNo ratings yet
- Pain Management-PRN OrdersDocument2 pagesPain Management-PRN OrdersMuhammad SaadNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CEBALLOS, Mary Kate L. (BSN 1-YA-18) - WEEK 2 LAB EXERCISE - Introduction To Human Anatomy and PhysiologyDocument6 pagesCEBALLOS, Mary Kate L. (BSN 1-YA-18) - WEEK 2 LAB EXERCISE - Introduction To Human Anatomy and PhysiologyKay ChoiNo ratings yet
- Spooky Scary SkeletonDocument6 pagesSpooky Scary SkeletonPiano Covers0% (1)
- 2 5388672510243898947 PDFDocument446 pages2 5388672510243898947 PDFDrAbdullah MehmoodNo ratings yet
- An Updated Approach To The Diagnosis of Myeloid Leukemia CutisDocument10 pagesAn Updated Approach To The Diagnosis of Myeloid Leukemia CutisfikriafisNo ratings yet
- Hemangiopericytoma of Palate A Rare Case ReportDocument4 pagesHemangiopericytoma of Palate A Rare Case ReportIJAR JOURNALNo ratings yet
- Veterinary Clinics: Large Trunk WoundsDocument26 pagesVeterinary Clinics: Large Trunk WoundsGuadalupe Cristina Chuchón CáceresNo ratings yet
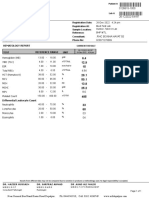
- BILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationDocument1 pageBILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationsaifNo ratings yet
- Floyd17 TB Ch12Document5 pagesFloyd17 TB Ch12sdjuknicNo ratings yet
- Lesson Plan Science Demo Junior HighDocument4 pagesLesson Plan Science Demo Junior HighDotecho Jzo Ey100% (1)
- Immunology of The Lymphatic System PDFDocument180 pagesImmunology of The Lymphatic System PDFCNPOULISNo ratings yet
- ScienceGeography3ResourceSample PDFDocument9 pagesScienceGeography3ResourceSample PDFmargantoniNo ratings yet
- Anatomy of A Frog ReadingDocument3 pagesAnatomy of A Frog ReadingRyan Carlo CondeNo ratings yet
- Muscular System MindmapDocument1 pageMuscular System MindmapMayeliz UrvinaNo ratings yet
- Effects of Myofascial Release and Stretching Technique On ROM and Reaction Time PDFDocument3 pagesEffects of Myofascial Release and Stretching Technique On ROM and Reaction Time PDFfisionovaisNo ratings yet
- BIOLOGY FORM 4 Chapter 2 PDFDocument18 pagesBIOLOGY FORM 4 Chapter 2 PDFadele30No ratings yet
- The Skeletal SystemDocument3 pagesThe Skeletal SystemMiguel GumatayNo ratings yet
- English For MedicineDocument52 pagesEnglish For MedicineRoya NaderiNo ratings yet
- The Functional Anatomy of PhonationDocument15 pagesThe Functional Anatomy of PhonationCarolyn BensonNo ratings yet
- Veterinary ImmunologyDocument20 pagesVeterinary ImmunologyJennifer Bumagat-BermudezNo ratings yet
- 10 TH Science Practical Guide EM PDFDocument15 pages10 TH Science Practical Guide EM PDFSRI VISHNUNo ratings yet
- ThyroidDocument7 pagesThyroidverawoNo ratings yet
- Fawcett The Cell Chapter 1Document38 pagesFawcett The Cell Chapter 1Mihnea ParaschivNo ratings yet
- CH 14 Brain & Cranial NervesDocument37 pagesCH 14 Brain & Cranial NervesHeather LaurenNo ratings yet
- CDU ZOOLOGY Anatomical Terminologies in Chordates and Vertebrates WorksheetDocument4 pagesCDU ZOOLOGY Anatomical Terminologies in Chordates and Vertebrates WorksheetKrisha Mae VillanuevaNo ratings yet
- 2 - Intro To ChordatesDocument19 pages2 - Intro To Chordatesapi-375285021No ratings yet
- Chist HidaticDocument25 pagesChist HidaticAna ScutelnicuNo ratings yet
- Cephalometric Lecture-1Document45 pagesCephalometric Lecture-1Batman 02053No ratings yet
- 9B Respiration - Gaseous Exchange in Man PDFDocument18 pages9B Respiration - Gaseous Exchange in Man PDFabdulrehman mughalNo ratings yet
- Erythroblastosis FetalisDocument4 pagesErythroblastosis FetalisGeorgina ErfeNo ratings yet