You might also like
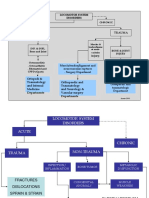
- Introduction of Musculosceletal Disorder and TraumaDocument19 pagesIntroduction of Musculosceletal Disorder and TraumaNdz1No ratings yet
- Jadwal Blok 5 Hema Dan ImunDocument10 pagesJadwal Blok 5 Hema Dan ImunNdz1No ratings yet
- Case Report Chrysomya Bezziana: Oral Myiasis Caused by in Anterior MaxillaDocument5 pagesCase Report Chrysomya Bezziana: Oral Myiasis Caused by in Anterior MaxillaNdz1No ratings yet
- Citation-51832066 RisDocument1 pageCitation-51832066 RisNdz1No ratings yet
- Overview Blok 5 Sistem Hematologi Dan ImmunologiDocument17 pagesOverview Blok 5 Sistem Hematologi Dan ImmunologiNdz1No ratings yet
- Pengobatan Pasien Tuberkulosis Paru dengan Multidrug Resistant (TB-MDRDocument13 pagesPengobatan Pasien Tuberkulosis Paru dengan Multidrug Resistant (TB-MDRNdz1No ratings yet
- Hipotiroid+ Nodul TiroidDocument61 pagesHipotiroid+ Nodul TiroidPuji AstutiNo ratings yet
- Periorificial Dermatitis in Children An Update and Description of A ChildDocument3 pagesPeriorificial Dermatitis in Children An Update and Description of A ChildNdz1No ratings yet
- Bone and NutritionDocument36 pagesBone and NutritionNdz1No ratings yet
- INTOLERANSI LAKTOSADocument9 pagesINTOLERANSI LAKTOSAmiraNo ratings yet
- Introduction of Musculosceletal Disorder and TraumaDocument19 pagesIntroduction of Musculosceletal Disorder and TraumaNdz1No ratings yet
- Revisi Blok 2 Kardioresp-2Document7 pagesRevisi Blok 2 Kardioresp-2Ndz1No ratings yet
- Introduction of Musculosceletal Disorder and TraumaDocument19 pagesIntroduction of Musculosceletal Disorder and TraumaNdz1No ratings yet
- Menu BazarDocument3 pagesMenu BazarNdz1No ratings yet
- HypertensionDocument37 pagesHypertensionNdz1No ratings yet
- Acute Heart Failure: Venice Chairiadi, MD, FIHADocument55 pagesAcute Heart Failure: Venice Chairiadi, MD, FIHANdz1No ratings yet
- 32 63 1 SMDocument5 pages32 63 1 SMNdz1No ratings yet
- 92 104 April Vol - 30 No - 2 2010 - 2Document13 pages92 104 April Vol - 30 No - 2 2010 - 2Paula CyntiaNo ratings yet
- 6334 12340 3 PBDocument7 pages6334 12340 3 PBNdz1No ratings yet
- 181 355 1 PBDocument6 pages181 355 1 PBRezy Arina PutriNo ratings yet
- Bakteri MuskuloskeletalDocument41 pagesBakteri MuskuloskeletalNdz1No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Year 9 Autumn 1 2018Document55 pagesYear 9 Autumn 1 2018andyedwards73No ratings yet
- B1 Mod 01 MathsDocument152 pagesB1 Mod 01 MathsTharrmaselan VmanimaranNo ratings yet
- Case Epidural HematomaDocument16 pagesCase Epidural HematomaBahRunNo ratings yet
- Narrative Techniques To Kill A MockingbirdDocument4 pagesNarrative Techniques To Kill A MockingbirdJoshua LawrenceNo ratings yet
- Supplement BDocument65 pagesSupplement BAdnan AsifNo ratings yet
- Learning Disabilities in The ClassroomDocument5 pagesLearning Disabilities in The ClassroomekielaszekNo ratings yet
- Webquest Biotechnology RubricDocument2 pagesWebquest Biotechnology Rubricapi-556285637No ratings yet
- Clinical Mental Health Counseling in Community and Agency Settings 5Th Edition Full ChapterDocument41 pagesClinical Mental Health Counseling in Community and Agency Settings 5Th Edition Full Chapterwilliam.kellar832100% (24)
- The Church of The Nazarene in The U.S. - Race Gender and Class in The Struggle With Pentecostalism and Aspirations Toward Respectability 1895 1985Document238 pagesThe Church of The Nazarene in The U.S. - Race Gender and Class in The Struggle With Pentecostalism and Aspirations Toward Respectability 1895 1985Luís Felipe Nunes BorduamNo ratings yet
- AthletesDocument494 pagesAthletesLuis CarlosNo ratings yet
- A Multivocal Literature Review of Decentralized Finance: Current Knowledge and Future Research AvenuesDocument37 pagesA Multivocal Literature Review of Decentralized Finance: Current Knowledge and Future Research Avenuesnofeh84660No ratings yet
- Lesson 3 Christianity ModuleDocument20 pagesLesson 3 Christianity ModuleCharmaine Alexi PaclibarNo ratings yet
- Regulation of Implantation and Establishment of Pregnancy in MammalsDocument271 pagesRegulation of Implantation and Establishment of Pregnancy in MammalsHelmer Hernán Sabogal Matias100% (1)
- Chisholm - Referring To Things That No Longer ExistDocument13 pagesChisholm - Referring To Things That No Longer ExistMichele Paolini PaolettiNo ratings yet
- Unit 01 Who Is A Contributor PDFDocument28 pagesUnit 01 Who Is A Contributor PDFKumpavatJayarajsinhNo ratings yet
- CS3C Mover Practice 2Document4 pagesCS3C Mover Practice 2Nguyễn Lê Hà ViNo ratings yet
- Chapter04 PDFDocument36 pagesChapter04 PDFBabuM ACC FIN ECONo ratings yet
- Antenna & Wave Propagation - Course OutlineDocument2 pagesAntenna & Wave Propagation - Course OutlineSabuj AhmedNo ratings yet
- Life Strategy 101: How To Live Live by Vision, Work With Purpose, and Achieve More SuccessDocument31 pagesLife Strategy 101: How To Live Live by Vision, Work With Purpose, and Achieve More SuccessMichelle Casto100% (2)
- ISO/IEC 20000 Lead Implementer Course (5 Days)Document3 pagesISO/IEC 20000 Lead Implementer Course (5 Days)rohitbanerjeeNo ratings yet
- Mars - Andrew D. Basiago - Letter To The Ngs - 12 12 08Document4 pagesMars - Andrew D. Basiago - Letter To The Ngs - 12 12 08Gavin SimmonsNo ratings yet
- Ethics Lecture Notes For Academic Year - Situation 1 Your Family Is An Exclusive Vacation On A - StuDocuDocument1 pageEthics Lecture Notes For Academic Year - Situation 1 Your Family Is An Exclusive Vacation On A - StuDocuRaveine JabatNo ratings yet
- CMT 565:waste and Wastewater Technology: Experiment No: 5 Title: Biochemical Oxygen Demand (Bod)Document4 pagesCMT 565:waste and Wastewater Technology: Experiment No: 5 Title: Biochemical Oxygen Demand (Bod)kuekNo ratings yet
- Rock and Roll and The American Dream: Essential QuestionDocument7 pagesRock and Roll and The American Dream: Essential QuestionChad HorsleyNo ratings yet
- PSM641UX TechnicalManua-V1.03Document128 pagesPSM641UX TechnicalManua-V1.03arulsethuNo ratings yet
- SPELD SA A Trip To The Top End-DSDocument16 pagesSPELD SA A Trip To The Top End-DSThien Tho NguyenNo ratings yet
- Grade 12 - MIL - Q1 - Week1 FinalDocument19 pagesGrade 12 - MIL - Q1 - Week1 FinalMa'am Regie Ricafort100% (2)
- Ebook Torrance (Dalam Stanberg) - 1-200 PDFDocument200 pagesEbook Torrance (Dalam Stanberg) - 1-200 PDFNisrina NurfajriantiNo ratings yet
- Definite IntegralsDocument51 pagesDefinite IntegralsKovid BalliNo ratings yet