You might also like
- Differential Diagnosis of The Diseases With Systolic MurmursDocument2 pagesDifferential Diagnosis of The Diseases With Systolic MurmursXiang Yun TanNo ratings yet
- Migne. Patrologiae Cursus Completus. Series Graeca. Volume 045.Document694 pagesMigne. Patrologiae Cursus Completus. Series Graeca. Volume 045.Patrologia Latina, Graeca et OrientalisNo ratings yet
- Plato, MetaphysicsDocument10 pagesPlato, MetaphysicsChristian CoseruNo ratings yet
- Migne. Patrologiae Cursus Completus. Series Graeca. Volume 004.Document564 pagesMigne. Patrologiae Cursus Completus. Series Graeca. Volume 004.Patrologia Latina, Graeca et Orientalis100% (1)
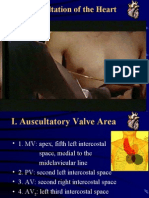
- Auscultation of HeartDocument92 pagesAuscultation of Heartsanjivdas100% (1)
- Migne. Patrologiae Cursus Completus. Series Graeca. Volume 046.Document654 pagesMigne. Patrologiae Cursus Completus. Series Graeca. Volume 046.Patrologia Latina, Graeca et Orientalis100% (1)
- Early Church History - Ecumenical Councils PDFDocument1,264 pagesEarly Church History - Ecumenical Councils PDFAaron TrujilloNo ratings yet
- Newman. Select Treatises of S. Athanasius, Archbishop of Alexandria: in Controversy With The Arians. 1842.Document352 pagesNewman. Select Treatises of S. Athanasius, Archbishop of Alexandria: in Controversy With The Arians. 1842.Patrologia Latina, Graeca et OrientalisNo ratings yet
- ST Mark of Ephesus On ST Gregory of Nyssa S Apokatastasis TeachingDocument4 pagesST Mark of Ephesus On ST Gregory of Nyssa S Apokatastasis TeachingDavid Minwoo Ewok KimNo ratings yet
- Psalm 120.2: Lying LipsDocument1 pagePsalm 120.2: Lying LipsMalcolm CoxNo ratings yet
- Canons of The Holy Fathers Assembled in The City of Nicæa in BithyniaDocument26 pagesCanons of The Holy Fathers Assembled in The City of Nicæa in BithyniaHadrian Mar Elijah Bar IsraelNo ratings yet
- FR Thomas Hopko - 55 MaximsDocument2 pagesFR Thomas Hopko - 55 MaximsAnina55No ratings yet
- The Veneration of The SaintsDocument6 pagesThe Veneration of The SaintsikonographicsNo ratings yet
- FC 33 ST John Chrysostom - Commentary - On - Saint - John - 01 - 47Document253 pagesFC 33 ST John Chrysostom - Commentary - On - Saint - John - 01 - 47ramona_anca_sv9232100% (1)
- MontanismDocument3 pagesMontanismalbertcook0% (1)
- Corpus MysticumDocument9 pagesCorpus MysticumCalisto MelibeuNo ratings yet
- Theodore the Studite's Defense of Icon VenerationDocument13 pagesTheodore the Studite's Defense of Icon VenerationMelangell Shirley Roe-Stevens Smith100% (1)
- Introduction To Gender ConceptsDocument12 pagesIntroduction To Gender ConceptsEunice OrtileNo ratings yet
- Second Council of Constantinople 553 AD Anathemas and Reincarnation CondemnedDocument24 pagesSecond Council of Constantinople 553 AD Anathemas and Reincarnation Condemnedcrdewitt100% (1)
- Hierarchies of Beings in The Patristic TDocument26 pagesHierarchies of Beings in The Patristic TStefi Gr100% (1)
- Patrologia GraecaDocument9 pagesPatrologia GraecaAlexandru Popovici0% (1)
- Standing or Kneeling To Receive Holy CommunionDocument23 pagesStanding or Kneeling To Receive Holy CommunionFrancis Lobo100% (1)
- What Is The Meaning of The Divine LiturgyDocument13 pagesWhat Is The Meaning of The Divine LiturgyjiorgosNo ratings yet
- Three New Hierarch (Service English)Document20 pagesThree New Hierarch (Service English)David Fotis CheungNo ratings yet
- Theodore Stoudite'sdefence of The Christ-Icon PDFDocument375 pagesTheodore Stoudite'sdefence of The Christ-Icon PDFMelangell Shirley Roe-Stevens SmithNo ratings yet
- From The NARTH Collected PapersDocument7 pagesFrom The NARTH Collected Papersenasoni23No ratings yet
- Byzantine Hesychasm in The 14th and 15thDocument55 pagesByzantine Hesychasm in The 14th and 15thGeorgel Rata100% (1)
- BABCOCK, William - Augustine and The Spirituality of DesireDocument21 pagesBABCOCK, William - Augustine and The Spirituality of DesireThiago Jordão100% (1)
- John Chryssavgis - Remembering Archbishop Stylianos HarkianakisDocument6 pagesJohn Chryssavgis - Remembering Archbishop Stylianos HarkianakisPanagiotis AndriopoulosNo ratings yet
- DeismDocument9 pagesDeismragusakaNo ratings yet
- Some Considerations On MusicDocument17 pagesSome Considerations On MusicDan ConstantinNo ratings yet
- Hallucinations: Natural vs. Drug-InducedDocument33 pagesHallucinations: Natural vs. Drug-InducedFitrio Citizen AntonyNo ratings yet
- On The Priesthood, ST Symeon Archbishop of ThessalonicaDocument11 pagesOn The Priesthood, ST Symeon Archbishop of Thessalonicaem43ver100% (1)
- Luther's View of Deification in Christ Through FaithDocument26 pagesLuther's View of Deification in Christ Through FaithcaralbertoNo ratings yet
- Turning East - Contemporary Philosophers and The Ancient Christian Faith (Rico Vitz)Document3 pagesTurning East - Contemporary Philosophers and The Ancient Christian Faith (Rico Vitz)vesteroseNo ratings yet
- Orthodox Wedding Guide for Saint Cyril ChurchDocument11 pagesOrthodox Wedding Guide for Saint Cyril ChurchAbouna David MorettiNo ratings yet
- Adrian Pabst - The Secularism of Post-Secularity - RIS 2012 - 2Document25 pagesAdrian Pabst - The Secularism of Post-Secularity - RIS 2012 - 2DanielNo ratings yet
- Windows to the KingdomDocument46 pagesWindows to the KingdomtudoradrianNo ratings yet
- Date For The Book of Revelation, The Testimony of The First ChristiansDocument4 pagesDate For The Book of Revelation, The Testimony of The First Christiansapi-3755336No ratings yet
- Es 14Document394 pagesEs 14carlodolciNo ratings yet
- 407 St. John ChrysostomDocument2 pages407 St. John ChrysostommedicalmatinsNo ratings yet
- Justin Martyrs Theory of Seminal Logos ADocument11 pagesJustin Martyrs Theory of Seminal Logos ARene OliverosNo ratings yet
- Blowers - Gentiles of The SoulDocument30 pagesBlowers - Gentiles of The Soulhobojoe9127No ratings yet
- The Kalam Cosmological Argument (INDEXED) - William Lane CraigDocument221 pagesThe Kalam Cosmological Argument (INDEXED) - William Lane CraigJoeMoellerNo ratings yet
- 5Document73 pages5Mark FrancisNo ratings yet
- AtheismDocument8 pagesAtheismScientiaveritatisNo ratings yet
- Thomas Arentzen Et Al - Byzantine Tree Life-Christianity and The Arboreal Imagination (2021)Document203 pagesThomas Arentzen Et Al - Byzantine Tree Life-Christianity and The Arboreal Imagination (2021)Koldo Gondra del CampoNo ratings yet
- New Directions in Evangelical Spirituality PDFDocument20 pagesNew Directions in Evangelical Spirituality PDFLucky Supit100% (1)
- Patristic Spirituality 2Document4 pagesPatristic Spirituality 2Evance JohanesNo ratings yet
- The Photian Schism: History and Legend of an Ecclesiastical ConflictDocument518 pagesThe Photian Schism: History and Legend of an Ecclesiastical ConflictKris BoçiNo ratings yet
- Trends in Eastern Orthodox Theological Anthropology: Towards A Theology of SexualityDocument10 pagesTrends in Eastern Orthodox Theological Anthropology: Towards A Theology of SexualityChristian WandriNo ratings yet
- Deskripsi MurmurDocument3 pagesDeskripsi MurmurLevina Tri RatanaNo ratings yet
- Principles Auscultatory Areas: ND NDDocument5 pagesPrinciples Auscultatory Areas: ND NDPinay YaunNo ratings yet
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- Heart Sounds and MurmursDocument38 pagesHeart Sounds and MurmursLaura Moise100% (5)
- Cardiac MurmursDocument53 pagesCardiac MurmursdrgashokNo ratings yet
- Cardiac MurmursDocument20 pagesCardiac MurmursFitri Nurullah100% (1)
- Heart SoundsDocument56 pagesHeart SoundsBetsy Babilonia100% (1)
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Heart & Neck Vessels Assessment: Kousar Perveen Assistant Professor The University of LahoreDocument46 pagesHeart & Neck Vessels Assessment: Kousar Perveen Assistant Professor The University of LahoreChenii RoyNo ratings yet
- Bio 9 Senses LabDocument9 pagesBio 9 Senses LabRobby Wiranata WijayaNo ratings yet
- Format Clock "After Hours"Document2 pagesFormat Clock "After Hours"Robby Wiranata WijayaNo ratings yet
- YOLLYDocument7 pagesYOLLYRobby Wiranata WijayaNo ratings yet
- Gis156 Slide Infeksi Parasit Usus Pada ManusiaDocument23 pagesGis156 Slide Infeksi Parasit Usus Pada ManusiaRobby Wiranata WijayaNo ratings yet
- Gis156 Slide Non Alcoholic Fatty Liver DiseaseDocument25 pagesGis156 Slide Non Alcoholic Fatty Liver DiseaseRobby Wiranata WijayaNo ratings yet
- Gangguan Sistem Perkemihan: DR A. Yuda Handaya, SPB, Finacs, FmasDocument132 pagesGangguan Sistem Perkemihan: DR A. Yuda Handaya, SPB, Finacs, FmasRobby Wiranata WijayaNo ratings yet
- Gagal Ginjal AkutDocument24 pagesGagal Ginjal AkutLia ZeniaNo ratings yet
- Asim & Shoaib (Gynae & Obs.) Biochemistry: D. Glucose-1, 6-BisphosphataseDocument12 pagesAsim & Shoaib (Gynae & Obs.) Biochemistry: D. Glucose-1, 6-BisphosphataseMedical TubeNo ratings yet
- Digitized Library Book ReproductionDocument575 pagesDigitized Library Book ReproductionMorgan Cabrera0% (1)
- 515Document972 pages515solecitodelmarazul100% (6)
- Assessing Children - Infancy Through Adolescence 1Document118 pagesAssessing Children - Infancy Through Adolescence 1kûrñï såñskrùthîNo ratings yet
- Kehamilan & Penyakit JantungDocument23 pagesKehamilan & Penyakit JantungSyifa NurainiNo ratings yet
- C2 ExamDocument29 pagesC2 ExamauNo ratings yet
- Congenital Heart DiseaseDocument124 pagesCongenital Heart DiseasemulkanmustafaNo ratings yet
- Interpretting Neonatal Xrays (Click Enable Macros)Document304 pagesInterpretting Neonatal Xrays (Click Enable Macros)John Phamnguyen100% (5)
- Medicine I - Topical Past Papers (2007-2019)Document50 pagesMedicine I - Topical Past Papers (2007-2019)Humna YounisNo ratings yet
- ACVIM Consensus of Myxomatous Mitral Valve Disease in DogsDocument14 pagesACVIM Consensus of Myxomatous Mitral Valve Disease in Dogssebas tianNo ratings yet
- Paediatrics Cardiology MCQDocument9 pagesPaediatrics Cardiology MCQJOYANTA ROY100% (1)
- Bos Specialty Assignment Cardiology-AmbroseDocument11 pagesBos Specialty Assignment Cardiology-Ambroseapi-396965096No ratings yet
- Acquired Heart DiseasesDocument41 pagesAcquired Heart DiseasesSaman SarKoNo ratings yet
- Cardiac CycleDocument14 pagesCardiac Cycleareznik3007No ratings yet
- IVMS ICM-Heart MurmursDocument22 pagesIVMS ICM-Heart MurmursMarc Imhotep Cray, M.D.No ratings yet
- QUESTIONS AND ANSWERS: CARDIOLOGY AND NEUROLOGYDocument117 pagesQUESTIONS AND ANSWERS: CARDIOLOGY AND NEUROLOGYMenna GalalNo ratings yet
- Pedia AbnormalDocument34 pagesPedia Abnormallight_tyrNo ratings yet
- Examining The PrecordiumDocument83 pagesExamining The PrecordiumnicolNo ratings yet
- MS MR As ArDocument21 pagesMS MR As ArTamim IshtiaqueNo ratings yet
- MCQ - Internal MedDocument2 pagesMCQ - Internal MedjennybongNo ratings yet
- Physical AssessmentDocument51 pagesPhysical AssessmentJasmin Jacob100% (2)
- Buzz WordsDocument8 pagesBuzz WordsSyed M AlamNo ratings yet
- UWORLD Notes April 29 2016 (Usmle Grassroots)Document80 pagesUWORLD Notes April 29 2016 (Usmle Grassroots)Bhuvana Usmle100% (3)
- Pocket Manual To Case TakingDocument72 pagesPocket Manual To Case Takingsandeep0% (1)
- Tiki Taka CK CardiologyDocument46 pagesTiki Taka CK CardiologyChristian Jara100% (2)
- Sample POMRDocument4 pagesSample POMRJeffrey RamosNo ratings yet
- Clinical Pediatrics MsMMaMDocument40 pagesClinical Pediatrics MsMMaMGoha Basha100% (3)
- Transposition of The Great Arteries PDFDocument6 pagesTransposition of The Great Arteries PDFSakuntalaPalanki100% (2)
- MRCP Classical Presentations PDFDocument427 pagesMRCP Classical Presentations PDFTank Tank67% (3)
- #5 Neonatal Cardiac AnomaliesDocument93 pages#5 Neonatal Cardiac AnomaliesSittie Hania100% (2)