You might also like
- 2, Facial Nerve ParalysisDocument23 pages2, Facial Nerve ParalysisSehar162No ratings yet
- Bell's Palsy: Submitted By: Twinkle Singh & Kinjalika VarmaDocument34 pagesBell's Palsy: Submitted By: Twinkle Singh & Kinjalika Varmatwinklestar1396No ratings yet
- Facial ParalysisDocument59 pagesFacial ParalysisSUnil Kumar100% (1)
- Bell's Palsy: Signs and SymptomsDocument9 pagesBell's Palsy: Signs and SymptomsMd.Sharifuzzaman FarabiNo ratings yet
- Bell's PalsyDocument25 pagesBell's PalsyGopi NathNo ratings yet
- Psoas AbscessDocument17 pagesPsoas AbscessYasinta HelenNo ratings yet
- Physical Examination 6Document95 pagesPhysical Examination 6Си Йи ФуNo ratings yet
- Disaster Management An OverviewDocument17 pagesDisaster Management An OverviewsivainamduguNo ratings yet
- Terapi Bells PalsyDocument38 pagesTerapi Bells Palsyshanaz100% (1)
- Acute Exacerbation Bronchial AsthmaDocument21 pagesAcute Exacerbation Bronchial AsthmaChekNatrahNo ratings yet
- AristocratDocument38 pagesAristocratTiến ThànhNo ratings yet
- Crohn's DiseaseDocument20 pagesCrohn's DiseaseTiffany AdriasNo ratings yet
- Can Stress Cause Bell's Palsy and Affect Its RecoveryDocument7 pagesCan Stress Cause Bell's Palsy and Affect Its RecoveryRoxan PacsayNo ratings yet
- Chronic Renal Failure: Dr. Ibrahiem SaeedDocument81 pagesChronic Renal Failure: Dr. Ibrahiem SaeedUzma KhanNo ratings yet
- Bells Palsy Slides 070214Document50 pagesBells Palsy Slides 070214Arif Nugroho SetiawanNo ratings yet
- Factors, Measures, and Problems of Quality Costs Program Implementation in The Manufacturing EnvironmentDocument6 pagesFactors, Measures, and Problems of Quality Costs Program Implementation in The Manufacturing EnvironmentFahad IzharNo ratings yet
- Thieves Booklet v12 Issuu Flat 2016Document16 pagesThieves Booklet v12 Issuu Flat 2016api-251091141No ratings yet
- Facialpain 150204113108 Conversion Gate01Document51 pagesFacialpain 150204113108 Conversion Gate01Muhammad IrfanNo ratings yet
- All PatternDocument4 pagesAll PatternManas BramheNo ratings yet
- The Cost of QualityDocument41 pagesThe Cost of QualityKundan Kumar SinghNo ratings yet
- Tianquan P-2: Heavenly SpringDocument1 pageTianquan P-2: Heavenly Springray72roNo ratings yet
- Spine Exam Lecture - Shaffer 2006Document65 pagesSpine Exam Lecture - Shaffer 2006মোহাম্মদ আবীরNo ratings yet
- A New Paradigm For Student LearnersDocument92 pagesA New Paradigm For Student LearnersTerry DoyleNo ratings yet
- Trigeminal Neuralgia in A Young Female Patient With V1 InvolementDocument19 pagesTrigeminal Neuralgia in A Young Female Patient With V1 Involement6ixSideCreate MNo ratings yet
- Cranial Nerves TransesDocument4 pagesCranial Nerves TransesChn PobadoraNo ratings yet
- The Peripheral Nervous SystemDocument80 pagesThe Peripheral Nervous SystemDanitra B AlexanderNo ratings yet
- Group 3 (Bell's Palsy)Document46 pagesGroup 3 (Bell's Palsy)gabrielle magdaraogNo ratings yet
- Acupressure Points To Stay FitDocument6 pagesAcupressure Points To Stay FitWafaa Abdel AzizNo ratings yet
- Neurologic ExaminationDocument67 pagesNeurologic Examinationሀይደር ዶ.ር100% (1)
- Si 9Document1 pageSi 9ray72roNo ratings yet
- Oleander Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineDocument13 pagesOleander Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineM KNo ratings yet
- A Patient With Big SpleenDocument24 pagesA Patient With Big SpleenWasswaNo ratings yet
- Accident Investigation 0Document49 pagesAccident Investigation 0pankajNo ratings yet
- Final Session Guide Root CauseDocument11 pagesFinal Session Guide Root CauseBagamel YlananNo ratings yet
- Fact Sheet Influenza Vaccine 2020 2021Document8 pagesFact Sheet Influenza Vaccine 2020 2021gsus17No ratings yet
- History TakingDocument40 pagesHistory TakingFaris FirasNo ratings yet
- G8DDocument61 pagesG8DRafi UdeenNo ratings yet
- Vision Technician FGDocument361 pagesVision Technician FGDr Anchal GuptaNo ratings yet
- Seminar: Facial Nerve PalsyDocument166 pagesSeminar: Facial Nerve PalsyShouvik ChowdhuryNo ratings yet
- The Basics of Disaster ResponseDocument100 pagesThe Basics of Disaster Responseমোঃ সাইদুর রহিম100% (1)
- EM - Emergency Management Summit Minneapolis 2014 Presentation - Surprise Prevention in Emergency Management - Eric WaageDocument19 pagesEM - Emergency Management Summit Minneapolis 2014 Presentation - Surprise Prevention in Emergency Management - Eric Waagee.RepublicNo ratings yet
- Noise in The Workplace: What You Should KnowDocument20 pagesNoise in The Workplace: What You Should KnowMumtaz AliNo ratings yet
- VERTIGODocument28 pagesVERTIGOdeni irawanNo ratings yet
- Cost of QualityDocument15 pagesCost of QualitySachin MethreeNo ratings yet
- Bell's Palsy - Treatment GuidelinesDocument4 pagesBell's Palsy - Treatment GuidelinessevattapillaiNo ratings yet
- Trigeminal NeurlgiaDocument5 pagesTrigeminal NeurlgiaAnonymous V1tCwPHlDNo ratings yet
- Department OF Physiotherapy: Bell'S PalsyDocument2 pagesDepartment OF Physiotherapy: Bell'S PalsybenjiNo ratings yet
- S O C R A T E S: History TakingDocument5 pagesS O C R A T E S: History Takingsnanan100% (1)
- 5 WhyDocument13 pages5 WhyPeter SzógaNo ratings yet
- Root Cause Analysis Template 41Document10 pagesRoot Cause Analysis Template 41Devi Chintya0% (1)
- Root Cause Investigation January 2 2018Document84 pagesRoot Cause Investigation January 2 2018Salman KhanNo ratings yet
- Scat EmptyDocument2 pagesScat Emptybuzank buzankNo ratings yet
- Migraine 2Document23 pagesMigraine 2danish sultanNo ratings yet
- What: Where (Location) : When (Date) : Who (Name) : HowDocument3 pagesWhat: Where (Location) : When (Date) : Who (Name) : HowDaniswara Krisna PrabathaNo ratings yet
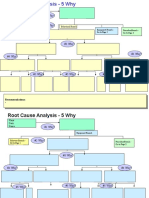
- Why Why AnalysisDocument20 pagesWhy Why AnalysisAmar ReddyNo ratings yet
- Liv 11Document1 pageLiv 11ray72roNo ratings yet
- CBL2 Facial Nerve RevDocument25 pagesCBL2 Facial Nerve RevtarshaNo ratings yet
- 125 Med Neuro Bell's PalsyDocument5 pages125 Med Neuro Bell's Palsyfire_n_iceNo ratings yet
- Bell' Palsy - PPT Report - PPT FINALDocument21 pagesBell' Palsy - PPT Report - PPT FINALCarshena Cuares100% (1)
- Facial Nerve Palsy - 111242Document12 pagesFacial Nerve Palsy - 111242Barath Kumar SinghNo ratings yet
- Suicide in The Islamic ViewDocument2 pagesSuicide in The Islamic ViewhesstyNo ratings yet
- INTUBASIDocument40 pagesINTUBASIhesstyNo ratings yet
- Stemi Mind MapDocument1 pageStemi Mind MaphesstyNo ratings yet
- Injuries To Traffic AccidentsDocument5 pagesInjuries To Traffic AccidentshesstyNo ratings yet
- Orthopaedic NeurologyDocument134 pagesOrthopaedic NeurologyRaymond Parung100% (1)
- Primary Trauma CareDocument39 pagesPrimary Trauma CareAzra Mesic100% (3)
- Experiment DesignDocument13 pagesExperiment DesignJnt100% (1)
- The Dreamtime ArticleDocument3 pagesThe Dreamtime Articlerich77No ratings yet
- Control and Coordination Class 10 Notes PDF Science Biology CBSEDocument5 pagesControl and Coordination Class 10 Notes PDF Science Biology CBSEgooode100% (2)
- Top 100 Diagnoses in Neurology Core Features, Synopses, IllustrationsDocument445 pagesTop 100 Diagnoses in Neurology Core Features, Synopses, IllustrationspondebernardoNo ratings yet
- Human Biology PASS Mid-Tri Exam Buster 2021Document12 pagesHuman Biology PASS Mid-Tri Exam Buster 2021Robert100% (1)
- Epilepsy in Pakistan - National Guidelines For Clinicians (Part 2)Document15 pagesEpilepsy in Pakistan - National Guidelines For Clinicians (Part 2)Fatima ShahidNo ratings yet
- Long Quiz AllDocument4 pagesLong Quiz AllMerben AlmioNo ratings yet
- Hepatic EncephalopathyDocument10 pagesHepatic Encephalopathymiss RN100% (1)
- Back To Basics: The Pathophysiology of Epileptic Seizures: A Primer For PediatriciansDocument12 pagesBack To Basics: The Pathophysiology of Epileptic Seizures: A Primer For Pediatriciansgerson altamiranoNo ratings yet
- WMS-IV Webinar September 2011 Handout PDFDocument23 pagesWMS-IV Webinar September 2011 Handout PDFMishal FatimaNo ratings yet
- 987556Document104 pages987556konrajNo ratings yet
- Brain Art Coloring Book f14Document3 pagesBrain Art Coloring Book f14api-261267976No ratings yet
- Advances in Cognitive Neurodynamics (VI)Document385 pagesAdvances in Cognitive Neurodynamics (VI)Víctor FuentesNo ratings yet
- Cranial Nerve ExaminationDocument6 pagesCranial Nerve ExaminationAlthea Aubrey AgbayaniNo ratings yet
- STOP, LOOK, AND LISTEN: The Challenge For Children With ADHDDocument13 pagesSTOP, LOOK, AND LISTEN: The Challenge For Children With ADHDJFNo ratings yet
- Social Anxiety Disorder Research PaperDocument7 pagesSocial Anxiety Disorder Research Paperapi-441382814No ratings yet
- The Intersectionality of Bipolar Disorder With Borderline Personality DisorderDocument14 pagesThe Intersectionality of Bipolar Disorder With Borderline Personality DisorderMuskaanNo ratings yet
- Eyes AssessmentDocument23 pagesEyes AssessmentAra AlibasaNo ratings yet
- Cheat Sheet: Responses Control of The Heart Rate Neurones & The Resting PotentialDocument1 pageCheat Sheet: Responses Control of The Heart Rate Neurones & The Resting PotentialLaila MahmudahNo ratings yet
- Dementia Nursing Care PlanDocument2 pagesDementia Nursing Care Planmp175767% (3)
- Physiology of Colour Vision 150731174500 Lva1 App6892Document40 pagesPhysiology of Colour Vision 150731174500 Lva1 App6892Shimaa HassanNo ratings yet
- Neuroacanthocytosis SyndromesDocument9 pagesNeuroacanthocytosis SyndromesBreiner PeñarandaNo ratings yet
- Memory and The Human Lifespan by Steve JoordensDocument130 pagesMemory and The Human Lifespan by Steve Joordenseva100% (2)
- HGD and Pedia Conditions-Outline PDFDocument23 pagesHGD and Pedia Conditions-Outline PDFAljhude Princess BernalesNo ratings yet
- 4 PDFDocument11 pages4 PDFHrishikesh BapatNo ratings yet
- LECTURE 9 - Pain-F17-4610.53-77 PDFDocument16 pagesLECTURE 9 - Pain-F17-4610.53-77 PDFJon DoeNo ratings yet
- Lord Chamberlain Rehab Brochure - WEBDocument2 pagesLord Chamberlain Rehab Brochure - WEBLisa BousquetNo ratings yet
- Binaural Frequency List GuideDocument30 pagesBinaural Frequency List GuideChristopher Parker100% (7)
- Unit 5: Control in Cells and in Organisms Chapters: Exam DatesDocument54 pagesUnit 5: Control in Cells and in Organisms Chapters: Exam DatesAsmaa AjajNo ratings yet
- 166 Serotonin SyndromeDocument5 pages166 Serotonin SyndromesayednourNo ratings yet