You might also like
- MRIDocument44 pagesMRIKumar Goutam100% (2)
- Radiology Physics: WWW - Krest.inDocument12 pagesRadiology Physics: WWW - Krest.inSivakumar SadasivamNo ratings yet
- MRI Bioeffects and SafetyDocument54 pagesMRI Bioeffects and SafetyYuda FhunkshyangNo ratings yet
- Radiology Recent AdvancesDocument66 pagesRadiology Recent AdvancesDr.P.NatarajanNo ratings yet
- MRI JointsDocument33 pagesMRI JointsMalaak BassamNo ratings yet
- (Philip T. English DCR, Christine Moore DCR (Auth.Document188 pages(Philip T. English DCR, Christine Moore DCR (Auth.Åri Budianto100% (1)
- CT PhysicsDocument19 pagesCT PhysicskrizzywhizzyNo ratings yet
- Mri SpineDocument64 pagesMri SpineWorthless BoysNo ratings yet
- Basic RadiologyDocument27 pagesBasic RadiologyHarmas Novryan FarezaNo ratings yet
- Doppler Ultrasonography of The Lower Extremity ArteriesDocument34 pagesDoppler Ultrasonography of The Lower Extremity ArteriesNidaa MubarakNo ratings yet
- MRI Design Guide April 2008: Section 1 Foreword & AcknowledgementsDocument61 pagesMRI Design Guide April 2008: Section 1 Foreword & AcknowledgementsPakka DostNo ratings yet
- Mri Master RodillaDocument9 pagesMri Master RodillaAndrea BelénNo ratings yet
- Skull XrayDocument35 pagesSkull XrayWebster The-TechGuy LunguNo ratings yet
- Fundamentals of MRI: Ysmael O. Alip, RRTDocument64 pagesFundamentals of MRI: Ysmael O. Alip, RRTGieDaquiuagNo ratings yet
- Clinical Radiology: The Thorax: Naveen Nair Gangadaran (0402005198)Document48 pagesClinical Radiology: The Thorax: Naveen Nair Gangadaran (0402005198)Chubii Luph DokhitNo ratings yet
- Radio 25 E1 Lec 10 MSK RadiologyDocument3 pagesRadio 25 E1 Lec 10 MSK RadiologyYavuz DanisNo ratings yet
- MRI of The Gastrointestinal Tract at High-Field Strength: Key PointsDocument12 pagesMRI of The Gastrointestinal Tract at High-Field Strength: Key PointsappleizANo ratings yet
- Evaluation and Routine Testing in Medical Imaging DepartmentsDocument18 pagesEvaluation and Routine Testing in Medical Imaging DepartmentsRankie Choi100% (1)
- Introduction To MRIDocument16 pagesIntroduction To MRIjuhiNo ratings yet
- Breast Symptoms - Algorithm For Imaging - Best Practice - Bisi - 2020 PDFDocument12 pagesBreast Symptoms - Algorithm For Imaging - Best Practice - Bisi - 2020 PDFBISI IndiaNo ratings yet
- Lecture Notes MRI (Part2)Document51 pagesLecture Notes MRI (Part2)cavronNo ratings yet
- CT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDocument7 pagesCT Angiography of The Lower Extremities The Peripheral Vascular System Presents Unique Imaging ChallengesDavid Puyó100% (1)
- Philips Learning Center Enewsletter Issue 3Document1 pagePhilips Learning Center Enewsletter Issue 3Suresh NarayanaswamyNo ratings yet
- Fast Spin Echo: Bioe 594 - Advanced Topics in Mri Nick GruszauskasDocument42 pagesFast Spin Echo: Bioe 594 - Advanced Topics in Mri Nick GruszauskasagithiaNo ratings yet
- Basics of Diffusion and Perfusion MRIDocument11 pagesBasics of Diffusion and Perfusion MRIPudhiavan AruviNo ratings yet
- Wiki TractographyDocument4 pagesWiki TractographynsurgphotoNo ratings yet
- Fundamentals of Diagnostic RadiologyDocument52 pagesFundamentals of Diagnostic RadiologyYabets100% (1)
- MR Requirements Musculoskeletal MRIDocument56 pagesMR Requirements Musculoskeletal MRIDifa ZafiraNo ratings yet
- Computer Aided Diagnosis DGDocument88 pagesComputer Aided Diagnosis DGosamahNo ratings yet
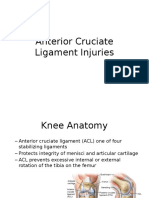
- Anterior Cruciate Ligament InjuriesDocument16 pagesAnterior Cruciate Ligament InjuriesAlmas PrawotoNo ratings yet
- Rapid ReportingDocument249 pagesRapid ReportingYuki NgNo ratings yet
- Approach To MRI Management in Stroke - PARI Kota MakassarDocument50 pagesApproach To MRI Management in Stroke - PARI Kota MakassarASMARNo ratings yet
- Basic Pulse SequencesDocument10 pagesBasic Pulse Sequencesjunghs2000No ratings yet
- 9 Skeletal SystemDocument63 pages9 Skeletal Systemvanderphys100% (1)
- CT ScanDocument5 pagesCT ScanAsdur KhanNo ratings yet
- ISUOG - Fetal Nervous System ExaminationDocument8 pagesISUOG - Fetal Nervous System ExaminationAzucenaNo ratings yet
- Updates Clinical: International Association For The Study of PainDocument6 pagesUpdates Clinical: International Association For The Study of PainSuaeni Kurnia WirdaNo ratings yet
- MRI Made EasyDocument97 pagesMRI Made EasyAlex EniuNo ratings yet
- MRI SafetyDocument42 pagesMRI SafetyadamayhalNo ratings yet
- MSK MRI Pulse SequencesDocument62 pagesMSK MRI Pulse SequencesOscar NogueraNo ratings yet
- MRI Lecture NotesDocument33 pagesMRI Lecture NotesBrandon44No ratings yet
- MRI PhysicsDocument113 pagesMRI PhysicsSaeed Ahmed ShaikhNo ratings yet
- Bone AgeDocument65 pagesBone AgeueumanaNo ratings yet
- AngiographyDocument17 pagesAngiographyPimsiree MameawNo ratings yet
- Body MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveDocument19 pagesBody MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveaegysabetterwayNo ratings yet
- MRI Safety Screening GuidlinesDocument5 pagesMRI Safety Screening GuidlinesEmi Murniati100% (1)
- Ultrasound TherapyDocument3 pagesUltrasound Therapyليلى مسلمة100% (1)
- Thesis Master ChartDocument18 pagesThesis Master ChartkavilankuttyNo ratings yet
- AXR Made EasyDocument13 pagesAXR Made EasycswathikanNo ratings yet
- Osteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Document45 pagesOsteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Saya MenangNo ratings yet
- CT KUB CN EditionDocument98 pagesCT KUB CN EditionphoenixibexNo ratings yet
- ESUR Guidelines On Contrast MediaDocument10 pagesESUR Guidelines On Contrast MediatsimitselisNo ratings yet
- Ultrasonography: Utrasonic DiagnosisDocument11 pagesUltrasonography: Utrasonic Diagnosisapi-3757838No ratings yet
- Chat GPTDocument2 pagesChat GPTGerardoMadrizNo ratings yet
- Women's Imaging: MRI with Multimodality CorrelationFrom EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownRating: 5 out of 5 stars5/5 (1)
- RF Coils for MRIFrom EverandRF Coils for MRIJ. Thomas VaughanNo ratings yet
- Introduction To Special Imaging ModalitiesDocument39 pagesIntroduction To Special Imaging ModalitiesIsaac ShirimaNo ratings yet
- Specialized Imaging Techniques 2010Document59 pagesSpecialized Imaging Techniques 2010John GreinerNo ratings yet
- ABFAS - Trauma Section Flashcards - QuizletDocument21 pagesABFAS - Trauma Section Flashcards - Quizletpjanu86No ratings yet
- Module 5 Surgical CriteriaDocument50 pagesModule 5 Surgical Criteriapjanu86No ratings yet
- Module 5 Surgical Criteria.Document53 pagesModule 5 Surgical Criteria.pjanu86No ratings yet
- Module 2 OrthopedicsDocument50 pagesModule 2 Orthopedicspjanu86No ratings yet
- Module 2 OrthopedicsDocument50 pagesModule 2 Orthopedicspjanu86No ratings yet
- Necrotizing Fasciitis: A Six-Year ExperienceDocument8 pagesNecrotizing Fasciitis: A Six-Year Experiencepjanu86No ratings yet
- Module 4 MedicineDocument50 pagesModule 4 Medicinepjanu86No ratings yet
- Ankle Ligaments On MRI: Appearance of Normal and Injured LigamentsDocument9 pagesAnkle Ligaments On MRI: Appearance of Normal and Injured Ligamentspjanu86No ratings yet
- Imaging of Sports Injuries in The Foot: James M. LinklaterDocument9 pagesImaging of Sports Injuries in The Foot: James M. Linklaterpjanu86No ratings yet
- Foot Ankle Spec 2008 Zgonis 46 53Document8 pagesFoot Ankle Spec 2008 Zgonis 46 53pjanu86No ratings yet
- CH 17-19 Learning ObjectivesDocument4 pagesCH 17-19 Learning Objectivespjanu86No ratings yet
- 6 VesselsDocument29 pages6 Vesselspjanu86No ratings yet
- Orthopaedic Study Guide 2014Document126 pagesOrthopaedic Study Guide 2014Yip Kar Jun100% (1)
- Charcot JointDocument8 pagesCharcot JointAtika SugiartoNo ratings yet
- Hospital Antibiotic Policy: ST Helens and Knowsley Hospitals TrustDocument72 pagesHospital Antibiotic Policy: ST Helens and Knowsley Hospitals TrustDimas RfNo ratings yet
- Non Odontogenic InfectionDocument38 pagesNon Odontogenic InfectionMuhamad ArifNo ratings yet
- Osteomyelitis: Steven K. SchmittDocument14 pagesOsteomyelitis: Steven K. SchmittYashinta MaharaniNo ratings yet
- Inflammatory Jaw LesionsDocument3 pagesInflammatory Jaw LesionsDeen MohdNo ratings yet
- Pathophysiology of OsteomyelitisDocument3 pagesPathophysiology of OsteomyelitisJhon Jerric Pante Aguinaldo100% (1)
- Prevention of Pin Site Infection in External FixatioDocument11 pagesPrevention of Pin Site Infection in External FixatioKim Gabrielle Exene LeeNo ratings yet
- Acute and Chronic OsteomyelitisDocument19 pagesAcute and Chronic OsteomyelitisEndy Destriawan0% (1)
- Neonatal InfectionDocument18 pagesNeonatal InfectionchinchuNo ratings yet
- Prometric Sample For DentistryDocument43 pagesPrometric Sample For DentistryAlvin RamirezNo ratings yet
- Pressure Ulcers and Wound CareDocument52 pagesPressure Ulcers and Wound CareKarina Mega WNo ratings yet
- CDC/NHSN Surveillance Definitions For Specific Types of InfectionsDocument30 pagesCDC/NHSN Surveillance Definitions For Specific Types of InfectionssofiaNo ratings yet
- Pulun: Template Case Based Scenario Examination (Cbse) 20/21Document52 pagesPulun: Template Case Based Scenario Examination (Cbse) 20/21SleepyHead ˋωˊNo ratings yet
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument11 pagesSummary of Product Characteristics: 4.1 Therapeutic IndicationsAninditaSahaNo ratings yet
- Bone and Joint InfectionDocument43 pagesBone and Joint Infectionraheeg siddigNo ratings yet
- Nutrition Case Study Presentation Slides - Jacob NewmanDocument27 pagesNutrition Case Study Presentation Slides - Jacob Newmanapi-283248618No ratings yet
- OSTEOMYELITISDocument28 pagesOSTEOMYELITISMuhammed sherbinNo ratings yet
- Nursing Care Plan-1idealDocument30 pagesNursing Care Plan-1idealSheila Mae PanisNo ratings yet
- Reported By: Sr. Jinggle U. Emata John Erick S Enero Calamba Doctors' CollegeDocument35 pagesReported By: Sr. Jinggle U. Emata John Erick S Enero Calamba Doctors' CollegeMarivic DianoNo ratings yet
- Dapus OrtopedDocument2 pagesDapus OrtopedqathrunnadaNo ratings yet
- What's New in Pediatric OrthopaedicsDocument8 pagesWhat's New in Pediatric OrthopaedicsDaniel AguilarNo ratings yet
- HemoglobinopathiesDocument10 pagesHemoglobinopathiespriscillaNo ratings yet
- CASE REPORT On OsteomyelitisDocument30 pagesCASE REPORT On OsteomyelitisNirbhay KatiyarNo ratings yet
- Antimicrobial StewardshipDocument37 pagesAntimicrobial StewardshipsamNo ratings yet
- Imaging Features of Pediatric Musculoskeletal Tuberculosis: Pictorial EssayDocument15 pagesImaging Features of Pediatric Musculoskeletal Tuberculosis: Pictorial EssayMarwin JouleNo ratings yet
- Week 6 SpondyloarthropathiesDocument124 pagesWeek 6 SpondyloarthropathiesJoeNo ratings yet
- Chronic Refractory Osteomyelitis of The Mandible and Maxilla Related To Dental Implant PlacementDocument4 pagesChronic Refractory Osteomyelitis of The Mandible and Maxilla Related To Dental Implant PlacementDiana BărbulescuNo ratings yet
- Official Program Superweek 2020Document9 pagesOfficial Program Superweek 2020Christian SagastumeNo ratings yet
- Etiology: Acute Hematogenous Osteomyelitis Subacute Osteomyelitis Chronic OsteomyelitisDocument42 pagesEtiology: Acute Hematogenous Osteomyelitis Subacute Osteomyelitis Chronic OsteomyelitisNoe-pal DynmNo ratings yet