You might also like
- Abnormalities of Haematopoiesis and Blood DisordersDocument51 pagesAbnormalities of Haematopoiesis and Blood DisordersRenad AlharbiNo ratings yet
- د رفل hematologicDocument60 pagesد رفل hematologicmuhammad.fajr.pharmacy96No ratings yet
- Clinical Pathology MCQs and Ansewrs PDFDocument29 pagesClinical Pathology MCQs and Ansewrs PDFAmeer MattaNo ratings yet
- List Blood Tests Performed As Part of A CBCDocument9 pagesList Blood Tests Performed As Part of A CBCamiosaNo ratings yet
- Quiz YourselfDocument154 pagesQuiz YourselfKandykane05100% (1)
- Hematopathology All LecturesDocument226 pagesHematopathology All LecturesYousif AlaaNo ratings yet
- Author(s) : John Levine License:Unless Otherwise Noted, This Material Is Made Available Under The TermsDocument50 pagesAuthor(s) : John Levine License:Unless Otherwise Noted, This Material Is Made Available Under The TermsMahda AzimahNo ratings yet
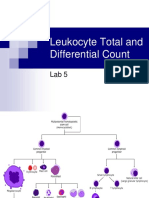
- Leukocyte Total and Differential CountDocument37 pagesLeukocyte Total and Differential CountHend HamedNo ratings yet
- An Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutDocument77 pagesAn Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutrhondreaNo ratings yet
- Wbcs Abnormalities: Muhammad Abrar Amin DVM 3 Year Cvas NarowalDocument25 pagesWbcs Abnormalities: Muhammad Abrar Amin DVM 3 Year Cvas NarowalMuhammad Abrar aminNo ratings yet
- Polycythemia VeraDocument4 pagesPolycythemia VeraAllyson VillarNo ratings yet
- Acute Lymphoid Leukemia (Airway Management)Document48 pagesAcute Lymphoid Leukemia (Airway Management)Ankita SamantaNo ratings yet
- Myeloproliferative DisorderDocument36 pagesMyeloproliferative DisorderKalpana ShahNo ratings yet
- A Complete Blood CountDocument6 pagesA Complete Blood CountecakimaNo ratings yet
- Physio PBLDocument13 pagesPhysio PBLCeejhay LeeNo ratings yet
- Anaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarDocument82 pagesAnaemi A: Joshi Abhishek Ashvinbhai F.Y.P.B.B.Sc - Nursing Govt - College of Nursing JamnagarReshu ThakuriNo ratings yet
- WaloDocument67 pagesWaloyepNo ratings yet
- Anaemia NNNNDocument82 pagesAnaemia NNNNAbdirahman Abdillahi Farah100% (1)
- How To Interpret HEMATOLOGY Test ResultsDocument36 pagesHow To Interpret HEMATOLOGY Test Resultssylvia haryantoNo ratings yet
- N 5315 Advaned Pathophysiology Anemia TranscriptDocument9 pagesN 5315 Advaned Pathophysiology Anemia TranscriptllukelawrenceNo ratings yet
- Hematology: 2021-University of Science A/Prof. Nguyen Thi HueDocument104 pagesHematology: 2021-University of Science A/Prof. Nguyen Thi HueMai Ly NguyễnNo ratings yet
- Circulatory System Part 1Document45 pagesCirculatory System Part 1Shivam0% (1)
- Hereditary AnemiaDocument77 pagesHereditary AnemiaAravindh SivaNo ratings yet
- S0850alug 1670953860959-SEU HDocument56 pagesS0850alug 1670953860959-SEU HAziz KhwajaNo ratings yet
- Anemia, Tic, DLC MbbsDocument50 pagesAnemia, Tic, DLC Mbbssharads221004No ratings yet
- XL22 - Basic HaematologyDocument18 pagesXL22 - Basic HaematologyAdi TrisnoNo ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Acute Lymphoid Leukemia (Case Presentation)Document48 pagesAcute Lymphoid Leukemia (Case Presentation)NEILVEL KNo ratings yet
- Heme-Onc Anki QDocument41 pagesHeme-Onc Anki Qjhk0428No ratings yet
- Problem Based Learning: Introductory To Clinical Hematology Omar Saffar 1Document14 pagesProblem Based Learning: Introductory To Clinical Hematology Omar Saffar 1Thabang ThaboNo ratings yet
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Manchester Blood PDFDocument9 pagesManchester Blood PDFShrouk EldakroryNo ratings yet
- Multiple Myeloma With PathophysiologyDocument32 pagesMultiple Myeloma With Pathophysiologymabec pagaduan90% (10)
- A Diagnostic Approach To Macrocytic AnemiaDocument87 pagesA Diagnostic Approach To Macrocytic AnemiaRathod arvinNo ratings yet
- Leukemias, Lymphomas, MyelomaDocument45 pagesLeukemias, Lymphomas, MyelomaYesyNo ratings yet
- Polycythemia VeraDocument8 pagesPolycythemia VeraSalam ZeeshanNo ratings yet
- Hematology: Mohamad H Qari, MD, FRCPADocument49 pagesHematology: Mohamad H Qari, MD, FRCPASantoz ArieNo ratings yet
- Megaloblastic AnemiaDocument13 pagesMegaloblastic AnemiaManchlaNo ratings yet
- Med Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsDocument36 pagesMed Surg Chapters 19 - 20 Hematologic Functions and Disorders PPT and QuestionsAshley100% (1)
- Kuliah LeukimiaDocument31 pagesKuliah LeukimiaMohammad SutamiNo ratings yet
- Hematology Lecture Notes PDFDocument102 pagesHematology Lecture Notes PDFMarisa IzzaNo ratings yet
- BLOOD AND ITS Diisorders - PPSXDocument18 pagesBLOOD AND ITS Diisorders - PPSXSwetamishraNo ratings yet
- Hematology Interest Group CNL Myeloproliferative NeoplasmDocument10 pagesHematology Interest Group CNL Myeloproliferative Neoplasmapi-384537137No ratings yet
- AnemiaDocument41 pagesAnemiabekthyNo ratings yet
- Current Diagnosis and Classification of Hematological MalignanciesDocument59 pagesCurrent Diagnosis and Classification of Hematological Malignanciesedel_herbityaNo ratings yet
- Interpretasi Darah RutinDocument22 pagesInterpretasi Darah Rutinboy jendri huluNo ratings yet
- Blood Lecture 2023fallDocument18 pagesBlood Lecture 2023falldodomrmr205No ratings yet
- Blood Histology: A. Prof Dr. Ruzanna DM, PHD, MSC, MDDocument23 pagesBlood Histology: A. Prof Dr. Ruzanna DM, PHD, MSC, MDHassoun hassoun100% (2)
- RBC Disorder 2Document9 pagesRBC Disorder 2Dongho ShinNo ratings yet
- Dr. Sazia NowshinDocument54 pagesDr. Sazia NowshinDanish GujjarNo ratings yet
- B HEMATLGY-ENsmallDocument43 pagesB HEMATLGY-ENsmallDean KharismaNo ratings yet
- Histo by DR - Ahmed Zahra (Blood)Document13 pagesHisto by DR - Ahmed Zahra (Blood)Abedelaal MohamedNo ratings yet
- DR Bambang - Anemia OverviewDocument263 pagesDR Bambang - Anemia OverviewOkta Dwi Kusuma AyuNo ratings yet
- Fast Facts: Leukemia: From initial gene mutation to survivorship supportFrom EverandFast Facts: Leukemia: From initial gene mutation to survivorship supportNo ratings yet
- Fast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaFrom EverandFast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaNo ratings yet
- Medicinal Plants: Tulsi (Ocimum Sanctum)Document4 pagesMedicinal Plants: Tulsi (Ocimum Sanctum)Muthu KumarNo ratings yet
- Endocrine Glands RevisedDocument47 pagesEndocrine Glands RevisedXyress Archer GosinganNo ratings yet
- Occult Meaning of Colours Purple Haze, All in My BrainDocument54 pagesOccult Meaning of Colours Purple Haze, All in My BrainrobinhoodlumNo ratings yet
- Neonatal JaundiceDocument56 pagesNeonatal Jaundicesuardiman acoNo ratings yet
- ENDODocument9 pagesENDOJohn denver FloresNo ratings yet
- Bio Lab ReportDocument7 pagesBio Lab Reportjoylee05No ratings yet
- Anticholinergic DrugsDocument19 pagesAnticholinergic DrugseashshankarNo ratings yet
- General Biology 1 NOTES PDFDocument18 pagesGeneral Biology 1 NOTES PDFRose Mendizabal82% (17)
- Bche 4090 1155168548Document7 pagesBche 4090 1155168548Yenny TsaiNo ratings yet
- Toltec Body Healing EbookDocument204 pagesToltec Body Healing EbookDanielle Grace100% (3)
- Experiment 33Document13 pagesExperiment 33KimNo ratings yet
- Effect of Plant Growth Enhancers On Growth and Flowering of Tuberose Cv. Prajwal PDFDocument4 pagesEffect of Plant Growth Enhancers On Growth and Flowering of Tuberose Cv. Prajwal PDFSupal DesaiNo ratings yet
- Comprehensive Head To Toe Assessment PDFDocument22 pagesComprehensive Head To Toe Assessment PDFVanessaMUellerNo ratings yet
- Vital SignsDocument3 pagesVital SignsNicole NipasNo ratings yet
- Chapter 18 - Apoptosis - 112612Document28 pagesChapter 18 - Apoptosis - 112612Anonymous nkR1PhIHNo ratings yet
- Golnic Lipidai Fingernails 000029915Document9 pagesGolnic Lipidai Fingernails 000029915Vita BūdvytėNo ratings yet
- Yoga ExercisesDocument10 pagesYoga ExercisesAna wulandariNo ratings yet
- Transcript of RecordsDocument3 pagesTranscript of Recordsmi5agencyNo ratings yet
- Melatonin Disturbances in Anorexia Nervosa and Bulimia NervosaDocument9 pagesMelatonin Disturbances in Anorexia Nervosa and Bulimia NervosaImelia AnggraeniNo ratings yet
- Comparative Anatomy Study of The Respiratory System Between Green Turtle (Chelonia Mydas) and Leatherback Turtle (Dermochelys Coriacea)Document1 pageComparative Anatomy Study of The Respiratory System Between Green Turtle (Chelonia Mydas) and Leatherback Turtle (Dermochelys Coriacea)AldinaNo ratings yet
- Manual Therapy For The Thorax - A Biomechanical Approach - D. Lee (DOPC, 1994) WW PDFDocument156 pagesManual Therapy For The Thorax - A Biomechanical Approach - D. Lee (DOPC, 1994) WW PDFEliMihaela100% (2)
- Urinalysis Results InterpretationDocument21 pagesUrinalysis Results InterpretationSutjipto WijonoNo ratings yet
- Adult Health Final Study GuideDocument5 pagesAdult Health Final Study GuideNurseNancy93100% (1)
- GastritisDocument10 pagesGastritisMario100% (2)
- (Criminalistics 5) Police Polygraphy (Lie-Detection)Document15 pages(Criminalistics 5) Police Polygraphy (Lie-Detection)Yam P Bustamante100% (2)
- Medical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manual DownloadDocument7 pagesMedical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manual DownloadSteven Dubose100% (24)
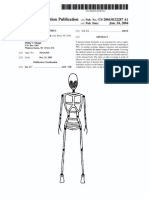
- Patente Endoesqueleto para Sex Doll SiliconaDocument12 pagesPatente Endoesqueleto para Sex Doll SiliconaGabriel De Jesus100% (1)
- 11 Chapter 1Document49 pages11 Chapter 1ram6025No ratings yet
- Form 86 - Health FormDocument1 pageForm 86 - Health Formbogtik100% (1)
- Apex o GenesisDocument54 pagesApex o GenesisbrahmannaNo ratings yet