You might also like
- Starting PositionsDocument60 pagesStarting Positionsheer rehman100% (1)
- Energy Conservation TechniquesDocument9 pagesEnergy Conservation Techniquesqwas zNo ratings yet
- Massachusetts - Protocols - 04.05.2019 - Cu Bookmarks PDFDocument557 pagesMassachusetts - Protocols - 04.05.2019 - Cu Bookmarks PDFMarius AlexandrescuNo ratings yet
- The Worst Mistake in The History of The Human Race - by Jared DiamondDocument4 pagesThe Worst Mistake in The History of The Human Race - by Jared DiamondwhychooseoneNo ratings yet
- Physiotherapy Management in Icu Patients: Dr.S.Ramachandran MPTDocument37 pagesPhysiotherapy Management in Icu Patients: Dr.S.Ramachandran MPTvaishnaviNo ratings yet
- Brunstorm'sDocument19 pagesBrunstorm'sHARSH 23 (Jalu)No ratings yet
- Foot and Ankle ArthrokinematicsDocument6 pagesFoot and Ankle ArthrokinematicsCraig StewartNo ratings yet
- Tennis Elbow ExerciseDocument2 pagesTennis Elbow Exercisedhirajkumar_1No ratings yet
- Cervical RadiculopathyDocument36 pagesCervical RadiculopathyAri SudarsonoNo ratings yet
- Hemiarthroplasty Hip - Apr20Document10 pagesHemiarthroplasty Hip - Apr20Shalu OjhaNo ratings yet
- Klumpke's ParalysisDocument7 pagesKlumpke's ParalysisNeelam VermaNo ratings yet
- Principles of Tendon Transfer in The Hand and ForearmDocument9 pagesPrinciples of Tendon Transfer in The Hand and Forearm'Ema Surya PertiwiNo ratings yet
- Ankle Fracture Rehab ProtocolDocument6 pagesAnkle Fracture Rehab Protocolbmj123No ratings yet
- StrokeDocument16 pagesStrokeFahmi AbdullaNo ratings yet
- Case of Peripheral Vascular Disease: Dr. Shresth ManglikDocument18 pagesCase of Peripheral Vascular Disease: Dr. Shresth ManglikShresth ManglikNo ratings yet
- Musculoskeletal RehabilitationDocument25 pagesMusculoskeletal RehabilitationNadia Ayu TiarasariNo ratings yet
- Physiotherapy After Hip HemiarthroplastyDocument7 pagesPhysiotherapy After Hip HemiarthroplastyMellow Moon RecordsNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- Gait AbnormalityDocument5 pagesGait AbnormalityKinshuk BansalNo ratings yet
- Hip DisorderDocument45 pagesHip DisorderMaryam KhalidNo ratings yet
- Coughing TechniqueDocument18 pagesCoughing TechniqueSiva ShanmugamNo ratings yet
- Physiological Response To Immobility and ActivityDocument14 pagesPhysiological Response To Immobility and ActivitywalterNo ratings yet
- Pes PlanusDocument6 pagesPes PlanusdeffyNo ratings yet
- Thoracic Surgeries: Types Description IndicationsDocument32 pagesThoracic Surgeries: Types Description IndicationsAnusha Verghese100% (1)
- Suspension Exercise TherapyDocument38 pagesSuspension Exercise TherapysudersonNo ratings yet
- Physiotherapy Management of Tennis Elbow................ ArticleDocument5 pagesPhysiotherapy Management of Tennis Elbow................ ArticleRupika SodhiNo ratings yet
- Periarthritis Shoulder By: DR - Sindhu.MPT (Ortho)Document39 pagesPeriarthritis Shoulder By: DR - Sindhu.MPT (Ortho)Michael Selvaraj100% (1)
- Pilates InserviceDocument11 pagesPilates InserviceToni MansfieldNo ratings yet
- Total Knee ReplacementDocument9 pagesTotal Knee ReplacementFaisal QureshiNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- PepDocument18 pagesPepAdrian DedicNo ratings yet
- FroDocument5 pagesFrochinmayghaisasNo ratings yet
- Postural, DrainageDocument7 pagesPostural, DrainageJames ThompsonNo ratings yet
- Chest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Document19 pagesChest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Physio EbookNo ratings yet
- Pes Cavus - PhysiopediaDocument10 pagesPes Cavus - PhysiopediavaishnaviNo ratings yet
- Introduction To Physiotherapy in General Surgical ConditionsDocument20 pagesIntroduction To Physiotherapy in General Surgical Conditionsakheel ahammedNo ratings yet
- Chest PhysiotherapyDocument12 pagesChest Physiotherapysenthilkumar100% (2)
- Therapeutic Exercise Foundation ConceptsDocument13 pagesTherapeutic Exercise Foundation ConceptsAngelic khanNo ratings yet
- Ankle Sprain AssessDocument18 pagesAnkle Sprain AssessFares EL DeenNo ratings yet
- Peripheral Vascular DiseaseDocument32 pagesPeripheral Vascular DiseaseShy PatelNo ratings yet
- Role of Physiotherapy in Management of Polio..seminarDocument14 pagesRole of Physiotherapy in Management of Polio..seminarAmandeep SinghNo ratings yet
- Cervical RibDocument15 pagesCervical RibArko duttaNo ratings yet
- PNF FullDocument46 pagesPNF FullHUZAIFA YAMAAN100% (1)
- Musculoskeletal TraumaDocument103 pagesMusculoskeletal TraumaJona Kristin EnclunaNo ratings yet
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDocument38 pagesJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalNo ratings yet
- Bicipital TendonitisDocument2 pagesBicipital TendonitisJ Cheung100% (2)
- Rehabilitation For Tennis ElbowDocument2 pagesRehabilitation For Tennis ElbowSamit Kumar Saha100% (1)
- Cervical PainDocument4 pagesCervical PainRhomadhoni Ika PutraNo ratings yet
- Pinky - Plantar FasciitisDocument34 pagesPinky - Plantar FasciitisRavindra choudharyNo ratings yet
- Diabetes and PhysiotherapyDocument15 pagesDiabetes and Physiotherapyane2saNo ratings yet
- Assessment of Gait Disorders in ChildrenDocument3 pagesAssessment of Gait Disorders in ChildrenMadalina RarincaNo ratings yet
- Pes Cavus: Eka Anggraini Padma Vidya GayatriDocument13 pagesPes Cavus: Eka Anggraini Padma Vidya GayatriPadma VidyaNo ratings yet
- Chest Pulmophysiothera PY: Prepared By: Floriza P. de Leon, PTRPDocument35 pagesChest Pulmophysiothera PY: Prepared By: Floriza P. de Leon, PTRPFloriza de LeonNo ratings yet
- Neuro AssessmentDocument6 pagesNeuro AssessmentfagpatelNo ratings yet
- Physical Therapy Clinic's Manual For The Most Common Cases: Dr. Yasser RefaaiDocument113 pagesPhysical Therapy Clinic's Manual For The Most Common Cases: Dr. Yasser RefaaiMaged Basha50% (2)
- Metatarsalgia: Yakshita Chaube B.P.T Final YearDocument18 pagesMetatarsalgia: Yakshita Chaube B.P.T Final YearKapil LakhwaraNo ratings yet
- Physiotherapy in Abdominal SurgeryDocument32 pagesPhysiotherapy in Abdominal SurgeryHUZAIFA YAMAANNo ratings yet
- Lung Expansion RevisionDocument89 pagesLung Expansion RevisionPatrick RoqueNo ratings yet
- Recent Advances in PhysiotherapyFrom EverandRecent Advances in PhysiotherapyCecily PartridgeNo ratings yet
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (2)
- TRIAGEDocument59 pagesTRIAGEagungNo ratings yet
- Nursing Trauma PDFDocument2 pagesNursing Trauma PDFagungNo ratings yet
- Spanish Pediatric Immunisation Reccommendation 2012Document23 pagesSpanish Pediatric Immunisation Reccommendation 2012agungNo ratings yet
- Chest PhysioDocument44 pagesChest PhysioagungNo ratings yet
- Medical Evacuation On TraumaDocument102 pagesMedical Evacuation On Traumaagung100% (1)
- Malnutrition Screening Tool - FINALDocument1 pageMalnutrition Screening Tool - FINALagungNo ratings yet
- Nursing TraumaDocument2 pagesNursing TraumaagungNo ratings yet
- Patient Transfer Inter-Departement Sheet Situation: Please Use Patient ID Label When AvailableDocument3 pagesPatient Transfer Inter-Departement Sheet Situation: Please Use Patient ID Label When AvailableagungNo ratings yet
- Emergenci NursingDocument2 pagesEmergenci NursingagungNo ratings yet
- DM 2Document85 pagesDM 2agungNo ratings yet
- GINA Pocket 2015Document32 pagesGINA Pocket 2015Ramzi AkramNo ratings yet
- Medical Evacuation On TraumaDocument102 pagesMedical Evacuation On Traumaagung100% (1)
- Triage PDFDocument59 pagesTriage PDFagungNo ratings yet
- GINA Pocket 2015Document32 pagesGINA Pocket 2015Ramzi AkramNo ratings yet
- Triage PDFDocument59 pagesTriage PDFagungNo ratings yet
- Medical Evacuation On TraumaDocument102 pagesMedical Evacuation On Traumaagung100% (1)
- Triage PDFDocument59 pagesTriage PDFagungNo ratings yet
- Patient - Safety and IT TrendsDocument3 pagesPatient - Safety and IT TrendsagungNo ratings yet
- Hand Hygiene Why How and When BrochureDocument7 pagesHand Hygiene Why How and When BrochureLeis FatwaNo ratings yet
- Manuskrip Bu Siwi PDFDocument18 pagesManuskrip Bu Siwi PDFagungNo ratings yet
- Manuskrip Bu Siwi PDFDocument18 pagesManuskrip Bu Siwi PDFagungNo ratings yet
- Fire Panel ZonesDocument2 pagesFire Panel ZonesagungNo ratings yet
- Ketiga 1 3 EngDocument14 pagesKetiga 1 3 EngAulia putriNo ratings yet
- HSCI130 Tutorial Exercise - Incidence & Prevalence ANSWER KEYDocument4 pagesHSCI130 Tutorial Exercise - Incidence & Prevalence ANSWER KEYarurojo100% (1)
- Diabetes and Virgin Coconut Oil DR Bruce FifeDocument3 pagesDiabetes and Virgin Coconut Oil DR Bruce Fifepetri_jv100% (1)
- Infected RPG SamplerDocument38 pagesInfected RPG SamplerEric Edesio100% (1)
- Community Health Nursing (CHN) - Heart of Nursing PH PDFDocument8 pagesCommunity Health Nursing (CHN) - Heart of Nursing PH PDFFahtma Irene Faye AnayatinNo ratings yet
- Atopic DermatitisDocument9 pagesAtopic DermatitisJorge De VeraNo ratings yet
- Induced SputumDocument6 pagesInduced Sputumnh2411No ratings yet
- Spiking Mortality Syndrome of ChickensDocument10 pagesSpiking Mortality Syndrome of ChickensDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (2)
- BDSDocument3 pagesBDScristalmae16No ratings yet
- Epidemiology and Etiology of Denture Stomatitis: KeywordsDocument10 pagesEpidemiology and Etiology of Denture Stomatitis: Keywordsluthfia choirunnisaNo ratings yet
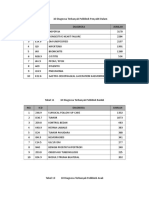
- 10 Diagnosa PenyakitDocument3 pages10 Diagnosa PenyakitDiny Rachma Putri HNo ratings yet
- Pork The Dangers of Pork Eating ExposedDocument13 pagesPork The Dangers of Pork Eating ExposedRajeb Bagasan DulunanNo ratings yet
- Heart WaterDocument3 pagesHeart WaterTorsten KnackstedtNo ratings yet
- EdemaDocument39 pagesEdemaMariyah Qibtiyyah Al JufriNo ratings yet
- Derma EmergencyDocument2 pagesDerma EmergencyAmirul Ashraf Bin ShukeriNo ratings yet
- Chartered Qualification in Human Resource Management: Group PresentationDocument20 pagesChartered Qualification in Human Resource Management: Group PresentationYazhini ManoharanNo ratings yet
- GAD-Narrative-2021 CECESDocument14 pagesGAD-Narrative-2021 CECESvengierose novalNo ratings yet
- Unit 1 Section 268 - 278Document9 pagesUnit 1 Section 268 - 278Nikhil Vinayakrao BajpaiNo ratings yet
- Lax - Toxin - The Cunning of Bacterial Poisons (Oxford, 2005)Document198 pagesLax - Toxin - The Cunning of Bacterial Poisons (Oxford, 2005)Pascaru OlegNo ratings yet
- Journal Reading ParuDocument53 pagesJournal Reading ParuDaniel IvanNo ratings yet
- Bahasa InggrisDocument2 pagesBahasa Inggriskhoirul ghofurNo ratings yet
- APSIC Guidelines For Environmental Cleaning and deDocument10 pagesAPSIC Guidelines For Environmental Cleaning and deKaterina NahampunNo ratings yet
- DA Strategic Plan Summary - Nov 7Document29 pagesDA Strategic Plan Summary - Nov 7Edward AdnanNo ratings yet
- Lecture 2Document3 pagesLecture 2Athena Thessa van VlotenNo ratings yet
- Oromia Region 2017 Meher Assessment Non Food Draft Report 20 Dec'17 - FDocument58 pagesOromia Region 2017 Meher Assessment Non Food Draft Report 20 Dec'17 - FMERHAWIT NEGATU100% (1)
- Miasm BerkshireDocument20 pagesMiasm Berkshirehyder2oo9No ratings yet
- EVRMC 1st EndorsementDocument4 pagesEVRMC 1st EndorsementPatrick DycocoNo ratings yet
- HematuriaDocument32 pagesHematuriaSurya Nirmala DewiNo ratings yet