You might also like
- Association Between MRNA Expression of Aromatase 1Document8 pagesAssociation Between MRNA Expression of Aromatase 1Nenny Yoanitha DjalaNo ratings yet
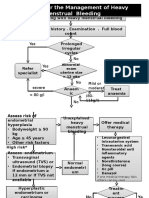
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNo ratings yet
- Estimated Fetal Weight Formula GuideDocument5 pagesEstimated Fetal Weight Formula GuideNenny Yoanitha Djala100% (1)
- En Endometrial Cancer Guide For PatientsDocument30 pagesEn Endometrial Cancer Guide For PatientsNenny Yoanitha DjalaNo ratings yet
- Hypertensionin PregnancyDocument100 pagesHypertensionin Pregnancyricky hutagalungNo ratings yet
- Night Shift Duty 11 FEBRUARIDocument2 pagesNight Shift Duty 11 FEBRUARINenny Yoanitha DjalaNo ratings yet
- Program Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Document1 pageProgram Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Nenny Yoanitha DjalaNo ratings yet
- AJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenDocument6 pagesAJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenNenny Yoanitha DjalaNo ratings yet
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaNo ratings yet
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNo ratings yet
- Termination Pregnancy Report 18 May 2010Document45 pagesTermination Pregnancy Report 18 May 2010Nenny Yoanitha DjalaNo ratings yet
- American Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFDocument6 pagesAmerican Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFNenny Yoanitha DjalaNo ratings yet
- Fetal and Maternal Effects of Forceps and VacuumDocument4 pagesFetal and Maternal Effects of Forceps and VacuumNenny Yoanitha DjalaNo ratings yet
- Medical Eligibility Criteria For Contraceptive Use Fifth Edition 2015Document14 pagesMedical Eligibility Criteria For Contraceptive Use Fifth Edition 2015agustinasntNo ratings yet
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaNo ratings yet
- Strategi Bisnis KorporasiDocument41 pagesStrategi Bisnis KorporasiAliMu'minHarahapNo ratings yet
- Final Data 2011 PDFDocument90 pagesFinal Data 2011 PDFNenny Yoanitha DjalaNo ratings yet
- Trali Dari Ats JournalDocument2 pagesTrali Dari Ats JournalNenny Yoanitha DjalaNo ratings yet
- Forceps Review in Modern Obstetric PracticeDocument5 pagesForceps Review in Modern Obstetric PracticeNenny Yoanitha DjalaNo ratings yet
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaNo ratings yet
- Anatomical Causes Bad Obstetric HistoryDocument3 pagesAnatomical Causes Bad Obstetric Historykyle31No ratings yet
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNo ratings yet
- Obstetrical Forceps - History Mystery and MoralityDocument16 pagesObstetrical Forceps - History Mystery and MoralityNenny Yoanitha DjalaNo ratings yet
- Forceps ExtractionDocument49 pagesForceps ExtractionNenny Yoanitha DjalaNo ratings yet
- Cytomegalovirus Infection in Patients With Active InflammatoryDocument7 pagesCytomegalovirus Infection in Patients With Active InflammatoryNenny Yoanitha DjalaNo ratings yet
- How To Explore After Forceps ExtractionDocument7 pagesHow To Explore After Forceps ExtractionNenny Yoanitha DjalaNo ratings yet
- Genetic Study of TORCH Infections in Women With BOH PDFDocument6 pagesGenetic Study of TORCH Infections in Women With BOH PDFNenny Yoanitha DjalaNo ratings yet
- Successful Pregnancy OutcomeDocument6 pagesSuccessful Pregnancy OutcomeNenny Yoanitha DjalaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Beth's PlightDocument9 pagesBeth's PlightyadmosheNo ratings yet
- NLRC Rules of Procedure 2011Document236 pagesNLRC Rules of Procedure 2011John Sowp MacTavishNo ratings yet
- Topic 5. Contemporary Approaches To MarketingDocument39 pagesTopic 5. Contemporary Approaches To MarketingFrancez Anne GuanzonNo ratings yet
- Bangsamoro Basic LawDocument36 pagesBangsamoro Basic LawMary Louisse RulonaNo ratings yet
- Challenges of Modern YouthDocument4 pagesChallenges of Modern YouthGautam VermaNo ratings yet
- Case For Analysis 6Document2 pagesCase For Analysis 6Micka OahNo ratings yet
- Warranty: Varian Medical Systems, X-Ray Products ("Varian") Warrants Its X-Ray Tubes ("X-Ray Tubes") As FollowsDocument2 pagesWarranty: Varian Medical Systems, X-Ray Products ("Varian") Warrants Its X-Ray Tubes ("X-Ray Tubes") As FollowsneohideNo ratings yet
- EAD-505-T3-Ethics QuizDocument6 pagesEAD-505-T3-Ethics QuizRaymond BartonNo ratings yet
- Indici Patient Portal Terms and Conditions v0 2 - 2Document3 pagesIndici Patient Portal Terms and Conditions v0 2 - 2hine1009No ratings yet
- Bartolome vs. SssDocument4 pagesBartolome vs. SssDario G. TorresNo ratings yet
- Architects Code of EthicsDocument2 pagesArchitects Code of EthicslynhareeNo ratings yet
- Engineering Ethics Theories ExplainedDocument43 pagesEngineering Ethics Theories ExplainedIgnatius TanNo ratings yet
- Magsalin Vs Coca-ColaDocument4 pagesMagsalin Vs Coca-ColaarciblueNo ratings yet
- Reading Sched and Correction Checklist 2022Document12 pagesReading Sched and Correction Checklist 2022Harry ۦۦNo ratings yet
- The Wilderness Society Style Guide 2014-2018Document52 pagesThe Wilderness Society Style Guide 2014-2018SaheemNo ratings yet
- The FFA Code of EthicsDocument1 pageThe FFA Code of EthicseaeastepNo ratings yet
- 4 Bidding Procedure For Consulting.09162016Document63 pages4 Bidding Procedure For Consulting.09162016Dustin FormalejoNo ratings yet
- 1 Contract Labour Act, 1970Document29 pages1 Contract Labour Act, 1970Satish SinhaNo ratings yet
- Construction Safety Seminar ReportDocument3 pagesConstruction Safety Seminar ReportfrancessichNo ratings yet
- Declaration forms for property and membership transferDocument3 pagesDeclaration forms for property and membership transferWelcome Real Estate ServicesNo ratings yet
- Understanding the Self and Teachings of St. AugustineDocument8 pagesUnderstanding the Self and Teachings of St. AugustineJowen Para CruzNo ratings yet
- Booking 03 28Document9 pagesBooking 03 28Bryan FitzgeraldNo ratings yet
- HCL TechnologiesDocument8 pagesHCL TechnologiesSai VasudevanNo ratings yet
- Moral Development Research PaperDocument7 pagesMoral Development Research Paperapi-329133700No ratings yet
- ExampleDocument1 pageExampleangelica villegasNo ratings yet
- Module 7 Paper - Consultants Report For Anywhere PD CapstoneDocument11 pagesModule 7 Paper - Consultants Report For Anywhere PD Capstoneapi-592769083No ratings yet
- The Meaning of Poverty: Draft - Please Treat AppropriatelyDocument35 pagesThe Meaning of Poverty: Draft - Please Treat AppropriatelyMaria GonzalesNo ratings yet
- Sen Po Ek Marketing Corporation Vs DigestDocument2 pagesSen Po Ek Marketing Corporation Vs DigestJessica BernardoNo ratings yet
- A Good Man Is Hard To Find - EditedDocument5 pagesA Good Man Is Hard To Find - Editedkevin MuthomiNo ratings yet
- Defense MechanismDocument19 pagesDefense MechanismMaricar Corina Canaya100% (1)