You might also like
- CASE REPORT 4: PNEUMONIA DEXTRA SUSPECT COVID-19 + ACUTE GASTRITISDocument17 pagesCASE REPORT 4: PNEUMONIA DEXTRA SUSPECT COVID-19 + ACUTE GASTRITISdianarahimmNo ratings yet
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Presus MalariaDocument66 pagesPresus MalariaAlchemistalazkaNo ratings yet
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- Pembahasan CBT COMBO 3Document802 pagesPembahasan CBT COMBO 3Sari Dewi WiratsihNo ratings yet
- Myelodisplastic SyndromeDocument9 pagesMyelodisplastic SyndromeEni JiantiNo ratings yet
- PuyerDocument1 pagePuyerjuliperNo ratings yet
- Jurding Nita Tka in RaDocument17 pagesJurding Nita Tka in RaNovitasariyantiNo ratings yet
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Tatalaksana Awal Koreksi Cairan pada Kasus SyokDocument60 pagesTatalaksana Awal Koreksi Cairan pada Kasus Syokmuhammad benyNo ratings yet
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNo ratings yet
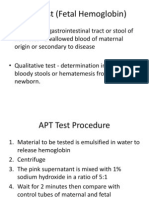
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- Iron Deficiency Anemia GuideDocument54 pagesIron Deficiency Anemia GuideRamsha ZafarNo ratings yet
- Laporan KasusDocument25 pagesLaporan KasusDidik Abdul RahmanNo ratings yet
- Disentri Et Causa Bacteria: Jl. Kutai Raya, Perumnas-3, Tangerang Kecamatan Curug, Kab. Tangerang, Provinsi Banten)Document14 pagesDisentri Et Causa Bacteria: Jl. Kutai Raya, Perumnas-3, Tangerang Kecamatan Curug, Kab. Tangerang, Provinsi Banten)Denny LeeNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Borang LohhDocument22 pagesBorang LohhRezki RamadhanNo ratings yet
- A Clinical Study of Etiology and Management of Acute Intestinal ObstructionDocument6 pagesA Clinical Study of Etiology and Management of Acute Intestinal ObstructionFalon PapalangiNo ratings yet
- Epista Ks IsDocument27 pagesEpista Ks IsCynthia MelindaNo ratings yet
- DRUG ERUPTION GUIDEDocument46 pagesDRUG ERUPTION GUIDESyahDikaNo ratings yet
- Final Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphDocument11 pagesFinal Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphwendryNo ratings yet
- Journal Reading THT - OMADocument15 pagesJournal Reading THT - OMAIndira MaycellaNo ratings yet
- Guide to Intraocular Cataract Extraction Techniques (ICCE ECCEDocument61 pagesGuide to Intraocular Cataract Extraction Techniques (ICCE ECCEBboy ToonNo ratings yet
- KARDIOMYOPATI: Understanding Heart Muscle DiseasesDocument28 pagesKARDIOMYOPATI: Understanding Heart Muscle DiseasesArif Zulfian MubarokNo ratings yet
- Geriatric Medicine KuliahDocument38 pagesGeriatric Medicine KuliahLia pramitaNo ratings yet
- Uremic LungDocument26 pagesUremic LungCitra Wulandari SofyanNo ratings yet
- Case Report on Pulmonary TuberculosisDocument38 pagesCase Report on Pulmonary TuberculosisBunga Listia ParamitaNo ratings yet
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaNo ratings yet
- Kegawatan Respirasi May2016-FkumyDocument62 pagesKegawatan Respirasi May2016-FkumyAgustina Tri P. DNo ratings yet
- RENAL EMERGENCIESDocument36 pagesRENAL EMERGENCIESPriscilla Christina NatanNo ratings yet
- Tata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoDocument84 pagesTata Laksana Sindroma Koroner Akut: Cholid Tri TjahjonoVio Alveolita PrimayaniNo ratings yet
- ClubfootDocument30 pagesClubfootdrusmanjamilhcmdNo ratings yet
- Bilas LambungDocument12 pagesBilas LambungNthie UnguNo ratings yet
- DIABETES MELITUS TYPE 2 MANAGEMENT UNDER 35 YEAR OLD WOMANDocument10 pagesDIABETES MELITUS TYPE 2 MANAGEMENT UNDER 35 YEAR OLD WOMANMeta SakinaNo ratings yet
- Diabetes Management & Insulin InitiationDocument39 pagesDiabetes Management & Insulin InitiationTaufiqurrochman Nur AminNo ratings yet
- Diagnosing Diabetes Insipidus with Dehydration, Water Deprivation, and Desmopressin TestsDocument17 pagesDiagnosing Diabetes Insipidus with Dehydration, Water Deprivation, and Desmopressin TestsM. RamazaliNo ratings yet
- Bimbingan UKMPPD - IPDDocument50 pagesBimbingan UKMPPD - IPDlinggarNo ratings yet
- Interpretasi Thorax FotoDocument38 pagesInterpretasi Thorax FotoMonika JonesNo ratings yet
- Journal ReadingDocument18 pagesJournal ReadingnafisyarifahNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Albumin in Liver Cirrhosis, SADocument37 pagesAlbumin in Liver Cirrhosis, SADwinita ViviantiNo ratings yet
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDocument16 pagesDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfNo ratings yet
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Seminar HD-RSUD Sleman 2019Document36 pagesSeminar HD-RSUD Sleman 2019herkamaya100% (1)
- CR Piopneumothoraks Nicky FIXdDocument62 pagesCR Piopneumothoraks Nicky FIXdPutri RahmawatiNo ratings yet
- Space-occupying lesions intracranial case reportDocument25 pagesSpace-occupying lesions intracranial case reportDiga Ana RusfiNo ratings yet
- Tachyarrhythmia SDocument46 pagesTachyarrhythmia SAsif HameedNo ratings yet
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilNo ratings yet
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahNo ratings yet
- Case Report: Urine Retention Et Causa Benign Hyperplasia ProstatDocument37 pagesCase Report: Urine Retention Et Causa Benign Hyperplasia ProstatKania A BustamNo ratings yet
- Interpreting ABG ResultsDocument28 pagesInterpreting ABG Resultsmafoel39No ratings yet
- Dr. Ago Harlim - MikosisDocument50 pagesDr. Ago Harlim - MikosisBrian Pasa NababanNo ratings yet
- Trantornos Anorrectales Adquiridos PDFDocument7 pagesTrantornos Anorrectales Adquiridos PDFIván Castellares RojasNo ratings yet
- Gagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanDocument20 pagesGagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanAdlan BinharyantoNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- Hypertension Management and Risk FactorsDocument41 pagesHypertension Management and Risk FactorsLeonardho Bayu WijayantoNo ratings yet
- Hypertension: Omaid Hayat KhanDocument35 pagesHypertension: Omaid Hayat KhanKhizraNo ratings yet
- BAGIAN ILMU PENYAKIT DALAM: HIPERTENSIDocument48 pagesBAGIAN ILMU PENYAKIT DALAM: HIPERTENSIRoberto SoehartonoNo ratings yet
- Kata PengantarDocument15 pagesKata PengantarSemestaNo ratings yet
- Referat TNDocument43 pagesReferat TNSemestaNo ratings yet
- Bone Infections: Acute, Subacute & Post-Op TypesDocument45 pagesBone Infections: Acute, Subacute & Post-Op TypesTasya Felicia MacellinNo ratings yet
- Data Base Clue and CUE Problem List Initial Diagnosis Planning Diagnosis Therapy Monitoring EducationDocument2 pagesData Base Clue and CUE Problem List Initial Diagnosis Planning Diagnosis Therapy Monitoring EducationnadiadhilaNo ratings yet
- DR Bangun RadiologiDocument135 pagesDR Bangun RadiologiSemestaNo ratings yet
- Biokimia ObesitasDocument54 pagesBiokimia ObesitassaidahrahmatNo ratings yet
- DR Is-Acute PancreatitisDocument11 pagesDR Is-Acute PancreatitisSemestaNo ratings yet
- Sistem Kolinergik ANSDocument53 pagesSistem Kolinergik ANSSemestaNo ratings yet
- DR Is-Acute Coronary SyndromeDocument23 pagesDR Is-Acute Coronary SyndromeSemestaNo ratings yet
- DR Tomy - Anatomi Organ EndokrinDocument41 pagesDR Tomy - Anatomi Organ EndokrinSemestaNo ratings yet
- Pathophysiology of Brain Injury and IschemiaDocument31 pagesPathophysiology of Brain Injury and IschemiaSemestaNo ratings yet
- DR Bambang EnsefalitisDocument46 pagesDR Bambang EnsefalitisSemestaNo ratings yet
- DR Bambang - Infant HypoglicemiaDocument97 pagesDR Bambang - Infant HypoglicemiaSemestaNo ratings yet
- DR Is-Acute Coronary SyndromeDocument23 pagesDR Is-Acute Coronary SyndromeSemestaNo ratings yet
- DR Nana MeningitisDocument44 pagesDR Nana MeningitisSemestaNo ratings yet
- Glomerulonephritis: Dr. Isbandiyah, SPPDDocument21 pagesGlomerulonephritis: Dr. Isbandiyah, SPPDMohammad SutamiNo ratings yet
- DR Is HipertensionDocument35 pagesDR Is HipertensionSemestaNo ratings yet
- Nephrotic Syndrome (NS) : Isbandiyah, DR, SPPDDocument19 pagesNephrotic Syndrome (NS) : Isbandiyah, DR, SPPDSemestaNo ratings yet
- DR Nana-Sindrom NefrotikDocument27 pagesDR Nana-Sindrom NefrotikSemestaNo ratings yet
- Leukemia: Dr. Isbandiyah SPPD Bag. Ilmu Penyakit Dalam Umm MalangDocument26 pagesLeukemia: Dr. Isbandiyah SPPD Bag. Ilmu Penyakit Dalam Umm MalangSemesta0% (1)
- HEPATOMADocument30 pagesHEPATOMASemestaNo ratings yet
- LymphomaDocument36 pagesLymphomaAnonymous 65zjdAVNo ratings yet
- DR Meddy LeukemiaDocument24 pagesDR Meddy LeukemiaSemestaNo ratings yet
- DR Isbandiyah HemostasisDocument30 pagesDR Isbandiyah HemostasisSemestaNo ratings yet
- Emergency Trauma & Non TraumaDocument60 pagesEmergency Trauma & Non TraumaSemestaNo ratings yet
- Dementia and Delirium - The Unrecognised Connection: Julia L. Poole CNC Aged CareDocument33 pagesDementia and Delirium - The Unrecognised Connection: Julia L. Poole CNC Aged CareAlfredo BambangNo ratings yet
- Etiologi DVT Pada Penerbangan Jarak Jauh Menurut EbmDocument32 pagesEtiologi DVT Pada Penerbangan Jarak Jauh Menurut EbmSemestaNo ratings yet
- Physilology of Kidney - F, S, R, EDocument24 pagesPhysilology of Kidney - F, S, R, ESemestaNo ratings yet
- Complications of Fractures and ManagementDocument65 pagesComplications of Fractures and ManagementSemestaNo ratings yet
- Avocado PDFDocument16 pagesAvocado PDFknot8No ratings yet
- Review Article: Greco-Arab and Islamic Herbal-Derived Anticancer Modalities: From Tradition To Molecular MechanismsDocument14 pagesReview Article: Greco-Arab and Islamic Herbal-Derived Anticancer Modalities: From Tradition To Molecular Mechanismsdragan_p2No ratings yet
- Dr. Sahar RakhshanfarDocument2 pagesDr. Sahar RakhshanfarsaharrakhshanfarinfNo ratings yet
- IL Companies Sep418Document6 pagesIL Companies Sep418Prasad RNNo ratings yet
- Cornell Notes Cognitive Dysfunction Klinefelter TurnerDocument5 pagesCornell Notes Cognitive Dysfunction Klinefelter TurnerBenNo ratings yet
- Discharge PlanDocument3 pagesDischarge PlanRoberto QuimsonNo ratings yet
- Scientific Research Journal of India (SRJI) Vol - 2, Issue - 1, Year - 2013Document59 pagesScientific Research Journal of India (SRJI) Vol - 2, Issue - 1, Year - 2013Dr. Krishna N. SharmaNo ratings yet
- New Microsoft Word DocumentDocument79 pagesNew Microsoft Word DocumentalexpharmNo ratings yet
- Causes and Management of Upper GI BleedingDocument4 pagesCauses and Management of Upper GI BleedingRazi HaiderNo ratings yet
- HydrocephalusDocument17 pagesHydrocephalusapi-265714286No ratings yet
- 3d Echo CardiologyDocument19 pages3d Echo CardiologyKanika JainNo ratings yet
- HackYourFitness PDFDocument17 pagesHackYourFitness PDFslslslslNo ratings yet
- Ineffective Breathing PatternDocument8 pagesIneffective Breathing PatternJansen Arquilita Rivera100% (2)
- SFDA Requirement For DEXADocument9 pagesSFDA Requirement For DEXAEhsan alwafaaNo ratings yet
- Zanki Renal PathologyDocument134 pagesZanki Renal Pathologysmian08No ratings yet
- Laisps Scientific Papers - Erotic TerrorDocument11 pagesLaisps Scientific Papers - Erotic Terrorjenny_tanseyNo ratings yet
- Nursing Care For Patient Undergoing TAHBSO For Ovarian GrowthDocument4 pagesNursing Care For Patient Undergoing TAHBSO For Ovarian Growthsugarmontejo83% (6)
- Effect of Age, Gender, and Sun Exposure On Ethnic Skin Photoaging: Evidence Gathered Using A New Photonumeric ScaleDocument6 pagesEffect of Age, Gender, and Sun Exposure On Ethnic Skin Photoaging: Evidence Gathered Using A New Photonumeric ScaleRiefka Ananda ZulfaNo ratings yet
- Cis Self-Study Lesson Plan: Instruments For Total Knee ArthroplastyDocument3 pagesCis Self-Study Lesson Plan: Instruments For Total Knee Arthroplastyjerimiah_manzonNo ratings yet
- Treating Fibroids With TCM PDFDocument13 pagesTreating Fibroids With TCM PDFshamim hijama100% (3)
- III Assessment For Well-Being APGAR SCORE - Dr. Virginia ApgarDocument30 pagesIII Assessment For Well-Being APGAR SCORE - Dr. Virginia ApgarKennethCallosNo ratings yet
- Chromosomes & Human GeneticsDocument78 pagesChromosomes & Human GeneticsBiil Dpo100% (1)
- Kayla Brockway Final ResumeDocument2 pagesKayla Brockway Final Resumeapi-457922767No ratings yet
- Prof. Eman Rushdy Sulphonylurea A Golden Therapy For DiabetesDocument51 pagesProf. Eman Rushdy Sulphonylurea A Golden Therapy For Diabetestorr123No ratings yet
- Microscopic ExaminationDocument72 pagesMicroscopic ExaminationbubblyeivinejNo ratings yet
- An Approach To A Case of PCOS/PCOD Through Homoeopathic Medicine ThyroidinumDocument13 pagesAn Approach To A Case of PCOS/PCOD Through Homoeopathic Medicine ThyroidinumHomoeopathic Pulse100% (1)
- Acupuncture Core Therapy: Shakujyū ChiryōDocument15 pagesAcupuncture Core Therapy: Shakujyū ChiryōFernando IglesiasNo ratings yet
- AdhdDocument8 pagesAdhdOkta SiregarNo ratings yet
- Level Worksheet: 2 DripDocument3 pagesLevel Worksheet: 2 DripDiksha AhluwaliaNo ratings yet
- Secondary SyphilisDocument2 pagesSecondary SyphilisRoberto López MataNo ratings yet