You might also like
- AnthropologyDocument17 pagesAnthropologyEliza AmandoNo ratings yet
- Addiction Group No.5)Document20 pagesAddiction Group No.5)Eliza AmandoNo ratings yet
- AttachmentDocument26 pagesAttachmentEliza AmandoNo ratings yet
- 4Document24 pages4Eliza AmandoNo ratings yet
- Demographic Transition in IranDocument17 pagesDemographic Transition in Iran5joanNo ratings yet
- Human Growth and DevelopmentDocument21 pagesHuman Growth and DevelopmentEliza AmandoNo ratings yet
- 2 Admit-Discharge ReasonsDocument1 page2 Admit-Discharge ReasonsEliza AmandoNo ratings yet
- Unemployment: Econ 151 - Macroeconomics Instructor: Bob DipaoloDocument44 pagesUnemployment: Econ 151 - Macroeconomics Instructor: Bob DipaoloEliza AmandoNo ratings yet
- DBRG 2018 English-Color WEBDocument2 pagesDBRG 2018 English-Color WEBAngel Lisette LaoNo ratings yet
- Bled PPT Ch15 Part03Document15 pagesBled PPT Ch15 Part03Eliza AmandoNo ratings yet
- Population PyramidsDocument45 pagesPopulation PyramidsEliza AmandoNo ratings yet
- Multiple Choice Questions: Chronic Obstructive Pulmonary Disease and Anaesthesia Anaesthesia For Awake CraniotomyDocument4 pagesMultiple Choice Questions: Chronic Obstructive Pulmonary Disease and Anaesthesia Anaesthesia For Awake CraniotomyEliza AmandoNo ratings yet
- Medication AdministrationDocument12 pagesMedication AdministrationDinah RealNo ratings yet
- Part One: Multiple Choice Questions (MCQ) (25 Marks)Document15 pagesPart One: Multiple Choice Questions (MCQ) (25 Marks)CeeNo ratings yet
- MSC .DP Abiud James Kuwijira 2015Document105 pagesMSC .DP Abiud James Kuwijira 2015Eliza AmandoNo ratings yet
- Guidelines Standards&criteria072010 PDFDocument37 pagesGuidelines Standards&criteria072010 PDFEliza AmandoNo ratings yet
- KC Vce H&HD U3&4 4e c06 WeDocument46 pagesKC Vce H&HD U3&4 4e c06 WeEliza AmandoNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- KC Vce H&HD U3&4 4e c06 WeDocument46 pagesKC Vce H&HD U3&4 4e c06 WeEliza AmandoNo ratings yet
- RDP3Document85 pagesRDP3Eliza AmandoNo ratings yet
- RDP3Document85 pagesRDP3Eliza AmandoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ascaris Suum PDFDocument6 pagesAscaris Suum PDFAdinda RahmaNo ratings yet
- Annotated BibliographyDocument31 pagesAnnotated BibliographyLara MelissaNo ratings yet
- Short Stories For KidsDocument14 pagesShort Stories For KidsSherine Lois QuiambaoNo ratings yet
- 5 - Circulation GraysDocument33 pages5 - Circulation GraysdrmanojkulNo ratings yet
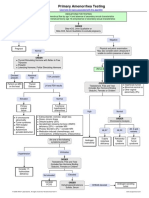
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmGabriella AguirreNo ratings yet
- Great Andamanese Lexicon EnglishDocument65 pagesGreat Andamanese Lexicon EnglishSai VenkateshNo ratings yet
- Effect of Adding Different Levels of Olive Leaf Powder To The Diet On The Production Performance and Some Physiological Characteristics of BroilersDocument9 pagesEffect of Adding Different Levels of Olive Leaf Powder To The Diet On The Production Performance and Some Physiological Characteristics of BroilersreviewjreNo ratings yet
- Cestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoDocument45 pagesCestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoMeylisa Gerson BayanNo ratings yet
- Respiratory Distress SyndromeDocument4 pagesRespiratory Distress SyndromeRommar RomeroNo ratings yet
- Are You Kidding MeDocument10 pagesAre You Kidding MeChelsea RoseNo ratings yet
- MATERNALDocument32 pagesMATERNALsean blaze100% (1)
- Development of The Fetal Membranes and PlacentaDocument4 pagesDevelopment of The Fetal Membranes and PlacentaBandula KusumsiriNo ratings yet
- ЧАРАКА-САМХИТА СУТРАСТХАНАDocument218 pagesЧАРАКА-САМХИТА СУТРАСТХАНАTremayne HansenNo ratings yet
- Nur112: Anatomy and Physiology ISU Echague - College of NursingDocument14 pagesNur112: Anatomy and Physiology ISU Echague - College of NursingWai KikiNo ratings yet
- Colors in The Human BodyDocument20 pagesColors in The Human Bodysarwarrosun100% (2)
- Metabolism and RelaxationDocument2 pagesMetabolism and RelaxationKrista BailieNo ratings yet
- Samphire2003 PDFDocument9 pagesSamphire2003 PDFYacine Tarik AizelNo ratings yet
- ECCO 2 Hemodynamics TestDocument3 pagesECCO 2 Hemodynamics TestpamoralesNo ratings yet
- Cheat Sheet 2Document2 pagesCheat Sheet 2oushaNo ratings yet
- Uterovaginal ProlapseDocument16 pagesUterovaginal Prolapseapi-3705046100% (1)
- Friesen C4ST Amended Input HC Safety Code 6 - 140 Omitted Studies 224pDocument224 pagesFriesen C4ST Amended Input HC Safety Code 6 - 140 Omitted Studies 224pSeth BarrettNo ratings yet
- TonsillitisDocument3 pagesTonsillitisVina MuspitaNo ratings yet
- The Little Book of Sexual HappinessDocument40 pagesThe Little Book of Sexual Happinesswolf4853100% (2)
- Essay-Vegan Vs OmnivorousDocument3 pagesEssay-Vegan Vs OmnivorousStiven Diaz Florez100% (1)
- M S N 3Document23 pagesM S N 3Muhammad YusufNo ratings yet
- Microbiology Mnemonics: Study Online atDocument3 pagesMicrobiology Mnemonics: Study Online atKriselda May Torio100% (1)
- EsquistocitosDocument10 pagesEsquistocitoswillmedNo ratings yet
- 5937 Understanding Nonverbal Communication Guidebook PDFDocument116 pages5937 Understanding Nonverbal Communication Guidebook PDFSalomao RodriguesNo ratings yet
- The Physiological Changes of PregnancyDocument16 pagesThe Physiological Changes of PregnancycchaitukNo ratings yet
- CDCDocument168 pagesCDCKing4Real100% (1)