You might also like
- Acute Respiratory Infections in ChildrenDocument43 pagesAcute Respiratory Infections in ChildrenAgiana PratamaNo ratings yet
- Acute Respiratory Infections: Pneumonia Bronkiolitis Bronkitis AkutDocument60 pagesAcute Respiratory Infections: Pneumonia Bronkiolitis Bronkitis AkutIrfanNo ratings yet
- Acute Respiratory InfectionDocument32 pagesAcute Respiratory InfectionRinnaAyuNovitaSary100% (1)
- 3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsDocument35 pages3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsCharisma Tiara RessyaNo ratings yet
- IspaDocument30 pagesIspahary anggoroNo ratings yet
- M M M MDocument32 pagesM M M Mيان فلوNo ratings yet
- Infeksi Saluran Pernafasan Akut (ISPA) Fifi SpADocument36 pagesInfeksi Saluran Pernafasan Akut (ISPA) Fifi SpARetno TharraNo ratings yet
- PneumoniaDocument66 pagesPneumoniaumanantini06100% (1)
- Acute Respiratory Infections: PneumoniaDocument31 pagesAcute Respiratory Infections: PneumoniaAndy KumaraNo ratings yet
- Pneumonia: H. Ridwan M. Daulay Wisman Dalimunthe Rini S. DaulayDocument49 pagesPneumonia: H. Ridwan M. Daulay Wisman Dalimunthe Rini S. DaulayKhairani PutriNo ratings yet
- Risk Factors and Types of Pneumonia in ChildrenDocument31 pagesRisk Factors and Types of Pneumonia in ChildrenAnonymous 0SYzMqje2No ratings yet
- Patho Lect - An Overview of Bacterial and Viral Infections 3-03-2015Document36 pagesPatho Lect - An Overview of Bacterial and Viral Infections 3-03-2015Taimoor Ul HassanNo ratings yet
- Penyakit Saluran PernapasanDocument49 pagesPenyakit Saluran PernapasanElgitha BandasoNo ratings yet
- Diagnosis Pneumonia: M Sidhartani ZainDocument28 pagesDiagnosis Pneumonia: M Sidhartani ZainApriany Fitri SangajiNo ratings yet
- 1 - Tropical Lung Dise - 2020 - Hunter S Tropical Medicine and Emerging InfectioDocument7 pages1 - Tropical Lung Dise - 2020 - Hunter S Tropical Medicine and Emerging InfectioThaiz P.SNo ratings yet
- Pneumonia Seminar HKNDocument66 pagesPneumonia Seminar HKNMahendra Yogi SemaraNo ratings yet
- Pcap Didactics ChanDocument61 pagesPcap Didactics ChanValerie Anne BebitaNo ratings yet
- CSS BPDocument14 pagesCSS BPUlfa FitrianingsihNo ratings yet
- Topic 2. Dyspnea. Complecated Pneumonia in Children. - ShortDocument69 pagesTopic 2. Dyspnea. Complecated Pneumonia in Children. - ShortIbtissame BadadNo ratings yet
- Childhood Pneumonia Diagnosis and TreatmentDocument65 pagesChildhood Pneumonia Diagnosis and TreatmentYemata HailuNo ratings yet
- Pneumonia Minggu GMEDocument42 pagesPneumonia Minggu GMEEkaNo ratings yet
- Group 1 - Case PresentationDocument70 pagesGroup 1 - Case PresentationVeejay CervantesNo ratings yet
- The Wheezing Infant: Airway Problems in ChildrenDocument4 pagesThe Wheezing Infant: Airway Problems in ChildrenDenise DelaneyNo ratings yet
- Acute Respiratory InfectoonDocument39 pagesAcute Respiratory InfectoonMahesa RamadhiantoNo ratings yet
- Non Resolving Pneumonia: by DR - Lokesh.L.V Moderators DR Mohan - Rao AND DR UmamaheshwariDocument58 pagesNon Resolving Pneumonia: by DR - Lokesh.L.V Moderators DR Mohan - Rao AND DR Umamaheshwaridrlokesh100% (5)
- Chapter 1Document30 pagesChapter 1Ayro Business CenterNo ratings yet
- Case Study PcapDocument3 pagesCase Study PcapClaire PalaciosNo ratings yet
- Kul3 - Pneumonia Uby s2-2011Document175 pagesKul3 - Pneumonia Uby s2-2011Suci HerawatiNo ratings yet
- Bronchiolitis: Ms AnamDocument56 pagesBronchiolitis: Ms AnamdmaulidaNo ratings yet
- Pediatric Community-Acquired Pneumonia: Causes, Symptoms & TreatmentDocument43 pagesPediatric Community-Acquired Pneumonia: Causes, Symptoms & TreatmentRazel Kinette AzotesNo ratings yet
- Pneumonia Pathophysiology, Diagnosis and TreatmentDocument57 pagesPneumonia Pathophysiology, Diagnosis and TreatmentAnas FikriNo ratings yet
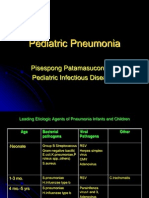
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDocument39 pagesPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputNo ratings yet
- Respiratory SystemDocument30 pagesRespiratory SystemHani El-asferNo ratings yet
- Pneumonia Symptoms and SignsDocument51 pagesPneumonia Symptoms and SignsArleen MatincaNo ratings yet
- Approachtocommonbacterial Infections:: Community-Acquired PneumoniaDocument17 pagesApproachtocommonbacterial Infections:: Community-Acquired PneumoniaFátima MartínezNo ratings yet
- Seminar ChildDocument28 pagesSeminar ChildAung Khaing MoeNo ratings yet
- InTech-Neonatal Pneumonia PDFDocument14 pagesInTech-Neonatal Pneumonia PDFClaudia PalominoNo ratings yet
- Pneumonia in Children & Lung AbscessDocument33 pagesPneumonia in Children & Lung AbscessAli JahidinNo ratings yet
- Respiratory Disease With Color AtlasDocument45 pagesRespiratory Disease With Color Atlasahmad shoaibNo ratings yet
- 01LongChap34 Pneumoniaandcomplications PDFDocument15 pages01LongChap34 Pneumoniaandcomplications PDFAngela Mitchelle NyanganNo ratings yet
- 3 - PneumoniaDocument6 pages3 - PneumoniaAmmar AlnajjarNo ratings yet
- Tuberculous Pleural Effusion GuideDocument12 pagesTuberculous Pleural Effusion GuideKarla DagdagNo ratings yet
- TuberculosisDocument76 pagesTuberculosissashmita rautNo ratings yet
- TBC Manula 2014Document47 pagesTBC Manula 2014Rhirin Fardianti AtmayasariNo ratings yet
- Blok 27 PertussisDocument36 pagesBlok 27 PertussisNiaaAprilita100% (1)
- Pulmonar y TuberculosisDocument35 pagesPulmonar y TuberculosistuyalimonNo ratings yet
- Hospital Acquired PneumoniaDocument48 pagesHospital Acquired PneumoniaKartika RezkyNo ratings yet
- PneumoniaDocument86 pagesPneumoniakhushisinghal.cse22No ratings yet
- READINGS PcapDocument2 pagesREADINGS PcapEden RelacionNo ratings yet
- Med - PPT Pneumonia For LectureDocument79 pagesMed - PPT Pneumonia For Lectureapi-3856051100% (23)
- Enteroviruses: Prepared By: Eriwan Osman Daban Azad Dastan Hadi Omer Ahmed Zanyar QadrDocument33 pagesEnteroviruses: Prepared By: Eriwan Osman Daban Azad Dastan Hadi Omer Ahmed Zanyar QadrDastan HadiNo ratings yet
- Antibiotics Training ManualDocument149 pagesAntibiotics Training ManualImran MullaNo ratings yet
- BronchitisDocument17 pagesBronchitisمیاں منیب احمدNo ratings yet
- Pneumonia: Practice GapDocument21 pagesPneumonia: Practice GaptamaNo ratings yet
- Infeksi Saluran Pernafasan BawahDocument38 pagesInfeksi Saluran Pernafasan BawahajenghalidaNo ratings yet
- DR As TuberculosisDocument59 pagesDR As TuberculosisAchhar SinghNo ratings yet
- 1100 - Lee PneumoniasDocument37 pages1100 - Lee PneumoniasAlejandro Kanito Alvarez SNo ratings yet
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- License KeysDocument2 pagesLicense KeyslslslslNo ratings yet
- Spo Internal BenchmarkingDocument2 pagesSpo Internal Benchmarkingmuhammad fadly100% (1)
- Book 1Document38 pagesBook 1Dewi AgustiniNo ratings yet
- Hand Hygiene LindaDocument40 pagesHand Hygiene LindaDewi AgustiniNo ratings yet
- No. Nama AlamatDocument38 pagesNo. Nama AlamatDewi AgustiniNo ratings yet
- Rational Use and Prevention of Antibiotic ResistanceDocument22 pagesRational Use and Prevention of Antibiotic ResistanceMD ASIFNo ratings yet
- MKSAP13-Pulmonary Medicine and Critical CareDocument85 pagesMKSAP13-Pulmonary Medicine and Critical CaresarfirazNo ratings yet
- Teaching Plan (Nephrotic Syndrome)Document4 pagesTeaching Plan (Nephrotic Syndrome)Dan Gerald Alcido SalungaNo ratings yet
- Cluster 5Document12 pagesCluster 5st. hyacinth radioNo ratings yet
- Elevated The Head of The Bed Assisted Change Position Every 2 Hours Encouraged Liberal Fluid IntakeDocument3 pagesElevated The Head of The Bed Assisted Change Position Every 2 Hours Encouraged Liberal Fluid IntakeDeinielle Magdangal RomeroNo ratings yet
- Antibiotic Prescribing Patterns at COVID-19 Dedicated Wards in Bangladesh: Findings From A Single Center StudyDocument5 pagesAntibiotic Prescribing Patterns at COVID-19 Dedicated Wards in Bangladesh: Findings From A Single Center Studyاحمد عرفاتNo ratings yet
- NP IvDocument36 pagesNP IvZharina VillanuevaNo ratings yet
- A.respiratory HistoryDocument3 pagesA.respiratory HistoryEl SpinnerNo ratings yet
- Ebook Cardiovascular and Pulmonary Physical Therapy Evidence To Practice 5Th Edition Frownfelter Test Bank Full Chapter PDFDocument24 pagesEbook Cardiovascular and Pulmonary Physical Therapy Evidence To Practice 5Th Edition Frownfelter Test Bank Full Chapter PDFEdwardStephensMDeqik100% (10)
- Swapan Kumar Nath Sanjay G Revankar Problem-Based PDFDocument1,163 pagesSwapan Kumar Nath Sanjay G Revankar Problem-Based PDFRestu100% (1)
- IPA 2011 Oral and Poster AbstractsDocument133 pagesIPA 2011 Oral and Poster AbstractsDarma YantieNo ratings yet
- Chest X-Ray Findings and Temporal Lung Changes in Patients With COVID-19 PneumoniaDocument9 pagesChest X-Ray Findings and Temporal Lung Changes in Patients With COVID-19 PneumoniaRaniNo ratings yet
- Approach To Common Respiratory DiseaseDocument57 pagesApproach To Common Respiratory DiseaseRajhmuniran KandasamyNo ratings yet
- Streptococcus Pneumoniae (Pneumococcus) - OverviewDocument4 pagesStreptococcus Pneumoniae (Pneumococcus) - OverviewstarykNo ratings yet
- Palliative Nursing Care PlanDocument5 pagesPalliative Nursing Care Planstudent_019No ratings yet
- 9 - Chapter 1. The Components of Quality in Health Care PDFDocument25 pages9 - Chapter 1. The Components of Quality in Health Care PDFJuanna Soehardy100% (2)
- CAP AlgorithmDocument1 pageCAP AlgorithmdamondouglasNo ratings yet
- SECTION I Inflammatory, Infective, and Congenital: Pyogenic Liver AbscessDocument12 pagesSECTION I Inflammatory, Infective, and Congenital: Pyogenic Liver AbscessandresNo ratings yet
- Presentation of DiptheriaDocument45 pagesPresentation of DiptheriaR-o-N-n-e-lNo ratings yet
- Name - Perumal Sex: M - AgeDocument21 pagesName - Perumal Sex: M - AgedrpravalkNo ratings yet
- Tri Kartika Setyarini, Aisyah Lahdji, Isna Zalwa Noor FajriDocument7 pagesTri Kartika Setyarini, Aisyah Lahdji, Isna Zalwa Noor Fajrisurya gunawanNo ratings yet
- Neonatal Pneumonia in Rural Bangladesh: Prevalence, Clinical Features and OutcomesDocument5 pagesNeonatal Pneumonia in Rural Bangladesh: Prevalence, Clinical Features and Outcomesmirashabrina12No ratings yet
- Helicobacter pylori flagella movementDocument52 pagesHelicobacter pylori flagella movementhema100% (1)
- Which Is The Primary Goal of Community Health Nursing?: NurseDocument87 pagesWhich Is The Primary Goal of Community Health Nursing?: NurseKish Dayanara GonzalesNo ratings yet
- ICD 10 Codes and Names for Common DiseasesDocument11 pagesICD 10 Codes and Names for Common DiseasesViki AY15No ratings yet
- TG Chapter01Document26 pagesTG Chapter01Gailstar GutierrezNo ratings yet
- Effects of Postural Drainage Physical Therapy Techniques On In-Patient Management of PneumoniaDocument4 pagesEffects of Postural Drainage Physical Therapy Techniques On In-Patient Management of PneumoniaSherlaz EfhalNo ratings yet
- Q-Bank (Micorbiology 1)Document102 pagesQ-Bank (Micorbiology 1)Ali DosaNo ratings yet
- Communicable Disease Nursing Post Test Questions & AnswersDocument3 pagesCommunicable Disease Nursing Post Test Questions & AnswersTomzki CornelioNo ratings yet
- Edit NG Drug StudyDocument35 pagesEdit NG Drug StudyAlleinad BarracasNo ratings yet