You might also like
- Cor Pulmonale Definition, Causes, Symptoms and TreatmentDocument13 pagesCor Pulmonale Definition, Causes, Symptoms and TreatmentRizki JaneldiNo ratings yet
- Cor Pulmonale: Dr. Gerrard UyDocument13 pagesCor Pulmonale: Dr. Gerrard UymuthiaraNo ratings yet
- Cor Pulmonale: Dr. Gerrard UyDocument13 pagesCor Pulmonale: Dr. Gerrard Uyfaridah azzah sariNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Manage and Diagnose Acute and Chronic Cor PulmonaleDocument42 pagesManage and Diagnose Acute and Chronic Cor PulmonaleNym Angga SantosaNo ratings yet
- Pulmonary HypertensionDocument54 pagesPulmonary HypertensionmendaimashokombaNo ratings yet
- Pemicu 6 Eko Blok KGDDocument128 pagesPemicu 6 Eko Blok KGDEko SiswantoNo ratings yet
- Pulmonary Hypertension: Saurabh Biswas PGT, Dept. of Chest Medicine, CNMCHDocument59 pagesPulmonary Hypertension: Saurabh Biswas PGT, Dept. of Chest Medicine, CNMCHbsaurabh20No ratings yet
- Heart Failure: Classification, Risk Factors and Clinical FeaturesDocument48 pagesHeart Failure: Classification, Risk Factors and Clinical FeaturesMaria Cristina Sierralta SimonNo ratings yet
- Cor PulmonaleDocument21 pagesCor Pulmonalemaibejose100% (1)
- KP 2.5.5.3 Cor PulmonaleDocument17 pagesKP 2.5.5.3 Cor Pulmonalenurul ramadhiniNo ratings yet
- 8) Chronic Cor PulmonaleDocument2 pages8) Chronic Cor PulmonaleAris PaparisNo ratings yet
- Pulmonary EmbolismDocument8 pagesPulmonary EmbolismspoilttbrattNo ratings yet
- Heart Failure: Classification, Risk Factors and Clinical FeaturesDocument28 pagesHeart Failure: Classification, Risk Factors and Clinical FeaturesfredyNo ratings yet
- Hypertensive Heart DiseaseDocument7 pagesHypertensive Heart DiseaseMirajwati AdikusumaNo ratings yet
- HEMODYNAMICSDocument28 pagesHEMODYNAMICSaries0411No ratings yet
- ModuleIV RespiratoryEmergencies CHF COPD AsthmaDocument96 pagesModuleIV RespiratoryEmergencies CHF COPD AsthmaSaiKiranNo ratings yet
- COR PULMONALE - MahasiswaDocument14 pagesCOR PULMONALE - MahasiswaGalih Maygananda PutraNo ratings yet
- Cor PulmonaleDocument19 pagesCor PulmonaleMartina RizkiNo ratings yet
- Congestive Heart Failure LathaDocument68 pagesCongestive Heart Failure LathaLatha GhanesanNo ratings yet
- Eisenmenger Syndrome: Clinical DefinitionDocument3 pagesEisenmenger Syndrome: Clinical Definition22194No ratings yet
- Pulmonary Edema: Prepared By: South West Education CommitteeDocument65 pagesPulmonary Edema: Prepared By: South West Education CommitteedanradulescuNo ratings yet
- Pulmonary HypertensionDocument36 pagesPulmonary HypertensionDiana_anca6100% (2)
- Cardiogenic Shock ManagementDocument66 pagesCardiogenic Shock ManagementdrkurniatiNo ratings yet
- Heart FailureDocument72 pagesHeart FailuremacNo ratings yet
- Cardiac Tamponade (Suryani)Document72 pagesCardiac Tamponade (Suryani)Hamdani UsmanNo ratings yet
- KOR PULMONAL Revisi Maret 2017 SGLDocument17 pagesKOR PULMONAL Revisi Maret 2017 SGLrumaisyah alkatiriNo ratings yet
- Pleno Minggu 3 Blok 3.2Document57 pagesPleno Minggu 3 Blok 3.2ima_nekonayagiNo ratings yet
- Cor Pulmonal and CHDDocument44 pagesCor Pulmonal and CHDamir iksanNo ratings yet
- Congestive Cardiac Failure GuideDocument61 pagesCongestive Cardiac Failure GuideYAMINIPRIYANNo ratings yet
- Zoom Final PA CathetherDocument45 pagesZoom Final PA Cathetherhasanafridi.mechNo ratings yet
- Evaluation and Management of Right-SidedDocument65 pagesEvaluation and Management of Right-SidedJevin JameriaNo ratings yet
- Pulmonary Emolism PresentationDocument17 pagesPulmonary Emolism PresentationKennedy Ng'andweNo ratings yet
- Cardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarDocument23 pagesCardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarD. Melba S.S ChinnaNo ratings yet
- Valvular Heart DiseaseDocument2 pagesValvular Heart DiseaseAnonymous TVk12eX4No ratings yet
- Cyanotic Heart DiseaseDocument47 pagesCyanotic Heart Disease87-Saranya MNo ratings yet
- New HematologyOncology FAE2016Document108 pagesNew HematologyOncology FAE2016omarNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- Respiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNDocument46 pagesRespiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNAboodsha ShNo ratings yet
- Cardiac Catheterization Hemodynamic Monitoring GuideDocument38 pagesCardiac Catheterization Hemodynamic Monitoring GuideMoch Irvan BadriNo ratings yet
- Pulmonary Heart DiseasesDocument26 pagesPulmonary Heart DiseasesmalekNo ratings yet
- Pulmonary Ventilation/Perfusion Relationships & DiagnosticsDocument38 pagesPulmonary Ventilation/Perfusion Relationships & DiagnosticsAbdallah AlasalNo ratings yet
- Pulmonary Hypertension: Causes, Diagnosis, Treatment and ClassificationDocument58 pagesPulmonary Hypertension: Causes, Diagnosis, Treatment and ClassificationDevashish VermaNo ratings yet
- Cyanotic Heart LesionsDocument40 pagesCyanotic Heart LesionsRaison D'etreNo ratings yet
- Ratheesh R.LDocument23 pagesRatheesh R.LvaishnaviNo ratings yet
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- COPD and Pulmonary Hypertension Cause Right Heart FailureDocument19 pagesCOPD and Pulmonary Hypertension Cause Right Heart FailureIka Lukita SariNo ratings yet
- Pulmonary Hypertension: An Overview of Causes, Symptoms and DiagnosisDocument40 pagesPulmonary Hypertension: An Overview of Causes, Symptoms and DiagnosisAlexander Santiago ParelNo ratings yet
- Acute Respiratory FailureDocument51 pagesAcute Respiratory Failureigorhorenko15No ratings yet
- Presentation 3Document14 pagesPresentation 3mbbs03032022No ratings yet
- In The Name of God: Cardiogenic Pulmonary EdemaDocument51 pagesIn The Name of God: Cardiogenic Pulmonary EdemaaldiansyahraufNo ratings yet
- V. Complications of CVDDocument26 pagesV. Complications of CVDJan Federick BantayNo ratings yet
- Pulmonary Vascular Disorders and Respiratory FailureDocument5 pagesPulmonary Vascular Disorders and Respiratory FailureTrishia GuillermoNo ratings yet
- Cor Pulmonale: Right Heart Failure Due to Lung DiseaseDocument62 pagesCor Pulmonale: Right Heart Failure Due to Lung DiseaseAlbert NixonNo ratings yet
- 4th Problem KGD DanielDocument130 pages4th Problem KGD DanielSelly HerliaNo ratings yet
- Approach To The Patient With Shortness of Breath: Colin EdwardsDocument37 pagesApproach To The Patient With Shortness of Breath: Colin EdwardsNur FadzilahNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument50 pagesCyanotic Congenital Heart DiseaseSasi KumarNo ratings yet
- Manage Acute Pulmonary Oedema in 38 CharactersDocument4 pagesManage Acute Pulmonary Oedema in 38 CharactersTze SiangNo ratings yet
- ECMO Cardiopulmonary Support in Critically Ill ChildrenDocument68 pagesECMO Cardiopulmonary Support in Critically Ill Childrenapi-3831614No ratings yet
- 281 481 1 SMDocument7 pages281 481 1 SMYuli MayasariNo ratings yet
- Cns Vascularization DR - Dianayu Hamama Pitra, SP.S, M.BiomedDocument43 pagesCns Vascularization DR - Dianayu Hamama Pitra, SP.S, M.BiomedHayaNo ratings yet
- ST Segment DepressiDocument16 pagesST Segment DepressiHayaNo ratings yet
- Drug Doses 2017Document127 pagesDrug Doses 2017Yuliawati HarunaNo ratings yet
- Parasit SkemaDocument12 pagesParasit SkemaFahlia Bena Pratama100% (1)
- Limping ChildDocument54 pagesLimping ChildHayaNo ratings yet
- Kelainan Kongenital Pada Tulang BelakangDocument16 pagesKelainan Kongenital Pada Tulang BelakangHayaNo ratings yet
- Neuro of Tal Molog IDocument42 pagesNeuro of Tal Molog IHayaNo ratings yet
- Kanker ServikDocument34 pagesKanker ServikRezky KotoNo ratings yet
- Diabetic Foot UlcerDocument33 pagesDiabetic Foot UlceragieajNo ratings yet
- Patogenesis ACSDocument124 pagesPatogenesis ACSHayaNo ratings yet
- Pathophysiology of HFDocument40 pagesPathophysiology of HFHayaNo ratings yet
- Digestion AnatomyDocument68 pagesDigestion Anatomysunil19854503No ratings yet
- Chest Injuries GuideDocument19 pagesChest Injuries GuideAbdi Kumala100% (1)
- Musculoskeletal tumor classification and treatmentDocument89 pagesMusculoskeletal tumor classification and treatmentHayaNo ratings yet
- Print Skill LabDocument1 pagePrint Skill LabHayaNo ratings yet
- Cryptorchidism Guide: Embryology, Causes, ClassificationDocument50 pagesCryptorchidism Guide: Embryology, Causes, ClassificationAlvin GfNo ratings yet
- Haya's English TaskDocument2 pagesHaya's English TaskHayaNo ratings yet
- Limping ChildDocument54 pagesLimping ChildHayaNo ratings yet
- Uro PrintDocument3 pagesUro PrintHayaNo ratings yet
- Colon 04Document28 pagesColon 04Yelsa NoritaNo ratings yet
- Dialogue SSDocument22 pagesDialogue SSHayaNo ratings yet
- SungsangDocument19 pagesSungsangHayaNo ratings yet
- English TaskDocument2 pagesEnglish TaskHayaNo ratings yet
- Print Skill LabDocument1 pagePrint Skill LabHayaNo ratings yet
- Sung SangDocument19 pagesSung SangHayaNo ratings yet
- Clinical Approach in NeuropathyDocument43 pagesClinical Approach in NeuropathyHayaNo ratings yet
- Dialogue SSDocument22 pagesDialogue SSHayaNo ratings yet
- Reaksi AnafilaksisDocument34 pagesReaksi AnafilaksisPutri Reno IntanNo ratings yet
- Inocencio School Student Health Declaration SheetDocument2 pagesInocencio School Student Health Declaration SheetCrunchy Fried RiceNo ratings yet
- Nursing Care Plan For Upper Resrpiratory Tract InfectionDocument2 pagesNursing Care Plan For Upper Resrpiratory Tract Infectionmariejo90% (30)
- Pneumothorax and lung lesions seen on chest X-raysDocument90 pagesPneumothorax and lung lesions seen on chest X-raysdsekulic_1100% (1)
- Kołtuniuk Et Al., 2017 PDFDocument11 pagesKołtuniuk Et Al., 2017 PDFDiba Eka DiputriNo ratings yet
- EMT NotesDocument58 pagesEMT NotesJosue PasillasNo ratings yet
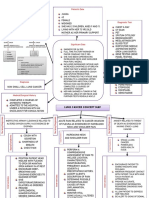
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- Clinical Practice Experience (CPE) Record 5 Phase 1Document11 pagesClinical Practice Experience (CPE) Record 5 Phase 1Sammy ChegeNo ratings yet
- Day 1. Mohd Sami 1Document67 pagesDay 1. Mohd Sami 1Baebee LouNo ratings yet
- Emergencies in Palliative CareDocument3 pagesEmergencies in Palliative CareJorge Cortina GonzalesNo ratings yet
- Penugasan B.ing (Ing)Document4 pagesPenugasan B.ing (Ing)ismail officialNo ratings yet
- Medical Surgical NursingDocument146 pagesMedical Surgical Nursingnisha jomonNo ratings yet
- Paed Osce ChecklistDocument40 pagesPaed Osce ChecklistLeCetraNo ratings yet
- ACUTE DECOMPENSATED HEART FAILUREDocument71 pagesACUTE DECOMPENSATED HEART FAILUREVivek Anandan100% (1)
- Devlin2020 PDFDocument8 pagesDevlin2020 PDFMatias FlammNo ratings yet
- Nursing considerations for clients on loop diuretics and beta blockersDocument59 pagesNursing considerations for clients on loop diuretics and beta blockersGil Raphael GanibanNo ratings yet
- TCAA's Safe Return-To-School Health PlanDocument12 pagesTCAA's Safe Return-To-School Health PlanGarfield The greatNo ratings yet
- Care of Patients With Noninfectious Lower Respiratory ProblemsDocument46 pagesCare of Patients With Noninfectious Lower Respiratory Problemsjrflores1284No ratings yet
- Respiratory System: Assessment: ObjectivesDocument19 pagesRespiratory System: Assessment: ObjectivesNURSES- NOOK & CORNERNo ratings yet
- Case # 4 Difficulty of BreathingDocument6 pagesCase # 4 Difficulty of BreathingGrace TanajuraNo ratings yet
- LP2 MAJOR EXAM 4 Files Merged 2 Files MergedDocument285 pagesLP2 MAJOR EXAM 4 Files Merged 2 Files MergedBianca ArceNo ratings yet
- Byssinosis-Health Hazards From Cotton DustDocument32 pagesByssinosis-Health Hazards From Cotton DustRajesh Dwivedi100% (1)
- Pratice Questions For NCLEX PDFDocument413 pagesPratice Questions For NCLEX PDFEmily97% (29)
- Nur 101 Data Base 1Document23 pagesNur 101 Data Base 1api-337919180No ratings yet
- PressedDocument71 pagesPressedGabriela ChristianNo ratings yet
- Andrade, Ban, Salleva - Liver Cirrhosis - Objectives, Manifestations, Drug StudyDocument9 pagesAndrade, Ban, Salleva - Liver Cirrhosis - Objectives, Manifestations, Drug StudyWindi Dawn SallevaNo ratings yet
- TB transmission, diagnosis, and treatmentDocument10 pagesTB transmission, diagnosis, and treatmentSahara Sahjz MacabangunNo ratings yet
- 1.5A Copd: OutlineDocument12 pages1.5A Copd: OutlineCecille Ann CayetanoNo ratings yet
- Assessment Planning Intervention Rationale Evaluation: Nursing DiagnosisDocument2 pagesAssessment Planning Intervention Rationale Evaluation: Nursing DiagnosisLovely CacapitNo ratings yet
- Professional Examination Board Group-2 Recruitment Test QuestionsDocument64 pagesProfessional Examination Board Group-2 Recruitment Test Questionsraghu051084No ratings yet
- COVID-19 Report on Virus Outbreak, Symptoms and TreatmentDocument16 pagesCOVID-19 Report on Virus Outbreak, Symptoms and TreatmentSara GuptaNo ratings yet