You might also like
- CBD Madya GastroDocument38 pagesCBD Madya GastroNurina yupiNo ratings yet
- The Perfect Keto Diet For Parkinson Disease:The Complete Guide To Treating And Managing Parkinson Disease With Delectable And Nourishing Keto Diet RecipesFrom EverandThe Perfect Keto Diet For Parkinson Disease:The Complete Guide To Treating And Managing Parkinson Disease With Delectable And Nourishing Keto Diet RecipesNo ratings yet
- Clinical Nutrition Conference Vision 2025Document22 pagesClinical Nutrition Conference Vision 2025Maya Rosmaria PNo ratings yet
- The Ideal Ulcerative Colitis Cookbook; The Superb Diet Guide To Relieving Symptoms And Preventing Complications Of Ulcerative Colitis, IBD, And Crohn's Disease With Nutritious Low-Fiber RecipesFrom EverandThe Ideal Ulcerative Colitis Cookbook; The Superb Diet Guide To Relieving Symptoms And Preventing Complications Of Ulcerative Colitis, IBD, And Crohn's Disease With Nutritious Low-Fiber RecipesNo ratings yet
- 10641Document38 pages10641Epi PanjaitanNo ratings yet
- Chronic Kidney Disease - UnhaluDocument57 pagesChronic Kidney Disease - UnhaluRahmawati HamudiNo ratings yet
- Prevent and Manage AKIDocument29 pagesPrevent and Manage AKImdonnyyuniarpratamaNo ratings yet
- Acid Peptic DisordersDocument67 pagesAcid Peptic DisordersTheop AyodeleNo ratings yet
- S18e - 1 10 2014Document300 pagesS18e - 1 10 2014Iuliana MariaNo ratings yet
- Lecture 1 - Replacing Renal Functions With Maintenance HD - Dr. GuecoDocument3 pagesLecture 1 - Replacing Renal Functions With Maintenance HD - Dr. GuecoElijah TeodosioNo ratings yet
- Diagnosing & Staging of Chronic Kidney Disease - WSAVA2009 - VINDocument5 pagesDiagnosing & Staging of Chronic Kidney Disease - WSAVA2009 - VINAnchang Don MaximNo ratings yet
- Case Discussion 1Document8 pagesCase Discussion 1Siraj INo ratings yet
- Diabetes: 2017-Ag-7750 Areej MinhasDocument16 pagesDiabetes: 2017-Ag-7750 Areej MinhasAreej Minhas RajputNo ratings yet
- Case Study (09 XT) Aspiration PnuemoniaDocument20 pagesCase Study (09 XT) Aspiration PnuemoniaChristy Rose AgrisNo ratings yet
- Clinical Teaching On MR Shine With Renal Calculi: Click To Edit Master Title StyleDocument25 pagesClinical Teaching On MR Shine With Renal Calculi: Click To Edit Master Title StyleDhanya RaghuNo ratings yet
- Canine Chronic Kidney Disease Current Diagnostics & Goals For Long-Term ManagementDocument7 pagesCanine Chronic Kidney Disease Current Diagnostics & Goals For Long-Term ManagementJuni ClaudiaNo ratings yet
- Jurnal CKDDocument7 pagesJurnal CKDJuni ClaudiaNo ratings yet
- Diabetes: 2017-Ag-7750 Areej MinhasDocument16 pagesDiabetes: 2017-Ag-7750 Areej MinhasAreej Minhas RajputNo ratings yet
- Renal FailureDocument56 pagesRenal FailureKoRnflakes100% (2)
- Gout Arthritis Dan PseudogoutDocument53 pagesGout Arthritis Dan PseudogoutCavaliere MascheratoNo ratings yet
- Case Study 4 Enteral FeedingDocument11 pagesCase Study 4 Enteral FeedingKISHORE KNo ratings yet
- Week 7 Kidney Disease: Sierra Parker, RD, LDN, CNSC, MBADocument38 pagesWeek 7 Kidney Disease: Sierra Parker, RD, LDN, CNSC, MBASierra ParkerNo ratings yet
- Parameter Penyakit Ginjal Kronis PentingDocument16 pagesParameter Penyakit Ginjal Kronis PentingMahdawwNo ratings yet
- Acute GastroenteritisDocument17 pagesAcute GastroenteritisClare Ducut100% (1)
- Renal Failure-Clinical CaseDocument35 pagesRenal Failure-Clinical Caseyaser773arfat2025No ratings yet
- Neonatal Cholestasis 2022 MPaeds Prep CourseDocument55 pagesNeonatal Cholestasis 2022 MPaeds Prep CourseTan Geok EngNo ratings yet
- Chronic Kidney InjuryDocument13 pagesChronic Kidney InjuryMaryam MohamedaliNo ratings yet
- Lecture 12. Nephrotic Syndrome, UTI in Children, Congenital Anomaly in Urinary SystemDocument30 pagesLecture 12. Nephrotic Syndrome, UTI in Children, Congenital Anomaly in Urinary SystemkrisnadewirahadiNo ratings yet
- Perforated Duodenal Ulcer Case StudyDocument45 pagesPerforated Duodenal Ulcer Case StudyJijie AzeeraNo ratings yet
- DM Puspa 2017Document22 pagesDM Puspa 2017hailysumartiNo ratings yet
- Diare Akut Pada Dewasa: Departemen Ilmu Penyakit Dalam FK UsuDocument37 pagesDiare Akut Pada Dewasa: Departemen Ilmu Penyakit Dalam FK Usuardi anharaksa yusuf100% (1)
- Neonatal Cholestasis: Priyanka VishwakarmaDocument38 pagesNeonatal Cholestasis: Priyanka VishwakarmaAlex100% (1)
- Case Presentation: by Femi Liz Sanjana AugusthyDocument31 pagesCase Presentation: by Femi Liz Sanjana AugusthyBlessyNo ratings yet
- LCR20070416B6Document2 pagesLCR20070416B6api-26938624No ratings yet
- VomitingDocument59 pagesVomitingزياد سعيدNo ratings yet
- CKD PresentationDocument51 pagesCKD PresentationBasneyatPragyanNo ratings yet
- CP On Abrutio PlacentaDocument13 pagesCP On Abrutio PlacentaUsha DeviNo ratings yet
- Chronic Kidney Diseases (CKD) - 2Document43 pagesChronic Kidney Diseases (CKD) - 2Victoria DadaNo ratings yet
- Cataract LectureDocument46 pagesCataract Lectureadelin litanNo ratings yet
- Diabetes Dan PJK, Farmasi DR - DjokoDocument39 pagesDiabetes Dan PJK, Farmasi DR - DjokoimbangNo ratings yet
- Lap LB 3 & PWSDocument446 pagesLap LB 3 & PWSfaridsubeqi22No ratings yet
- Chronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaDocument62 pagesChronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaSamuel LalNo ratings yet
- Acute Kidney Injury Etd Nov-Dec HPSF Sem 6 2022Document22 pagesAcute Kidney Injury Etd Nov-Dec HPSF Sem 6 2022Harry James Potter James PotterNo ratings yet
- CHRONIC DIRRHEA FinalDocument93 pagesCHRONIC DIRRHEA FinalAtifNo ratings yet
- Acute Pancreatitis Guide: Causes, Symptoms, Diagnosis and TreatmentDocument34 pagesAcute Pancreatitis Guide: Causes, Symptoms, Diagnosis and TreatmentDrscottmccallNo ratings yet
- Kidney Emergency: M. Syamsul BakhriDocument30 pagesKidney Emergency: M. Syamsul BakhrierahadeNo ratings yet
- IBD Ulcerative Colitis & Ghrons DiseaseDocument125 pagesIBD Ulcerative Colitis & Ghrons DiseaseDr. Ammar Khalil100% (2)
- Cholelithiasis and Liver CirrhosisDocument39 pagesCholelithiasis and Liver CirrhosisKate ValdesNo ratings yet
- Acute Glomerulonephritis Case StudyDocument6 pagesAcute Glomerulonephritis Case StudyjakerzNo ratings yet
- Chronic Kidney Disease Diagnosis, Stages, and ManagementDocument3 pagesChronic Kidney Disease Diagnosis, Stages, and ManagementPetrina XuNo ratings yet
- Bedah 21 Nov 2022 + FU 19 Nov 22 + Patof.Document28 pagesBedah 21 Nov 2022 + FU 19 Nov 22 + Patof.maya_rosmariaNo ratings yet
- Mini Case StudyDocument16 pagesMini Case Studyapi-534319171No ratings yet
- Secretory Diarrhea Caused by Pancreatic VIPomaDocument24 pagesSecretory Diarrhea Caused by Pancreatic VIPomaElaine June FielNo ratings yet
- Case Pres-CkdDocument21 pagesCase Pres-CkdKathleenNo ratings yet
- Diabetic KetoacidosisDocument26 pagesDiabetic Ketoacidosissalma.nasr003No ratings yet
- Renal FailureDocument31 pagesRenal Failureapi-195799092No ratings yet
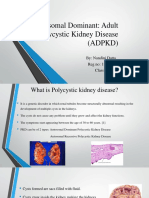
- ADPKD Causes, Symptoms and TreatmentDocument11 pagesADPKD Causes, Symptoms and TreatmentrutwickNo ratings yet
- CPG: Management of GoutDocument25 pagesCPG: Management of Goutadi_asrafNo ratings yet
- Aloe Vera: A Potential Herb and Its Medicinal ImportanceDocument25 pagesAloe Vera: A Potential Herb and Its Medicinal ImportanceSusan Sitha Irma YuhanitaNo ratings yet
- 4 5820951304909882278 PDFDocument386 pages4 5820951304909882278 PDFMohamed HamoodNo ratings yet
- Test bank medical surgical nursing in canada 5th edition lewisDocument57 pagesTest bank medical surgical nursing in canada 5th edition lewismarcuskenyatta275100% (1)
- Nausea A Review of Pathophysiology 2016Document15 pagesNausea A Review of Pathophysiology 2016Tony AndersonNo ratings yet
- Session #40 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Document6 pagesSession #40 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Ha Lec Finals ReviewerDocument28 pagesHa Lec Finals ReviewerKyutie KoNo ratings yet
- Family MedicineDocument288 pagesFamily MedicineSavitri15100% (2)
- Mental Health ResearchDocument3 pagesMental Health Researchlien adersonNo ratings yet
- 10 Super Healing Foods 2015 PDFDocument25 pages10 Super Healing Foods 2015 PDFJeromeHeadley100% (9)
- Traditional indian medicine.அகஸ்தியர் சித்த வைத்திய நிலையம் - AGASTHIAR ALL DIESEACESDocument26 pagesTraditional indian medicine.அகஸ்தியர் சித்த வைத்திய நிலையம் - AGASTHIAR ALL DIESEACESDeebaNo ratings yet
- Download Lewiss Medical Surgical Nursing Assessment And Management Of Clinical Problems 12Th Edition Mariann M Harding full chapterDocument68 pagesDownload Lewiss Medical Surgical Nursing Assessment And Management Of Clinical Problems 12Th Edition Mariann M Harding full chapterroy.saunders943100% (3)
- Food Protein-Induced Allergic Proctocolitis of Infancy - UpToDateDocument14 pagesFood Protein-Induced Allergic Proctocolitis of Infancy - UpToDateLisa MaNo ratings yet
- Gastrointestinal Root WordsDocument4 pagesGastrointestinal Root WordsPaula McAuliffeNo ratings yet
- Comprehensive Index to Find Musculoskeletal ConditionsDocument16 pagesComprehensive Index to Find Musculoskeletal ConditionsMustafa Ali0% (1)
- Full Download Test Bank For Medical Surgical Nursing in Canada 4th Edition Sharon L Lewis PDF Full ChapterDocument36 pagesFull Download Test Bank For Medical Surgical Nursing in Canada 4th Edition Sharon L Lewis PDF Full Chaptersaucisseserratedv8s97100% (20)
- Case StudyDocument22 pagesCase StudyBiway RegalaNo ratings yet
- Homoeopathic Remedies For Irritable Bowel Syndrome - Dr. Ks. Gopi - Pulse - LinkedinDocument7 pagesHomoeopathic Remedies For Irritable Bowel Syndrome - Dr. Ks. Gopi - Pulse - LinkedinsubratNo ratings yet
- Jurnal Colic AbdomenDocument5 pagesJurnal Colic AbdomenMadania PattyNo ratings yet
- Guideline For Medical Examination For Food Handlers in Fishery Industry in MalaysiaDocument11 pagesGuideline For Medical Examination For Food Handlers in Fishery Industry in Malaysiaibnu salimNo ratings yet
- Hospital Medicine Disease and Disorder List PDFDocument3 pagesHospital Medicine Disease and Disorder List PDFDevendraKumarNo ratings yet
- PPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieDocument98 pagesPPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieAnthony Hardie100% (5)
- Digestive Health Nursing Review QuestionsDocument37 pagesDigestive Health Nursing Review QuestionsNorPhea - នភាNo ratings yet
- Malabsorption and Elimination DisordersDocument120 pagesMalabsorption and Elimination DisordersBeBs jai SelasorNo ratings yet
- Solfeggio Chart Solfeggio Meditations by Glenn Harrold 1pg PDFDocument1 pageSolfeggio Chart Solfeggio Meditations by Glenn Harrold 1pg PDFMarkMadMunkiNo ratings yet
- Confidential GlaxoSmithKline Document Shows 36 Infant Deaths Following VaccinationDocument1,271 pagesConfidential GlaxoSmithKline Document Shows 36 Infant Deaths Following Vaccinationdiligentpurpose100% (2)
- Nutrition For Patients With Gastrointestinal Disorders Lec 7Document20 pagesNutrition For Patients With Gastrointestinal Disorders Lec 7Youssif Menam100% (1)
- Alistofsomeimportantmedicinalplantswiththeirmedicinalusesfrom Himalayan State Uttarakhand IndiaDocument12 pagesAlistofsomeimportantmedicinalplantswiththeirmedicinalusesfrom Himalayan State Uttarakhand IndiaSTKNo ratings yet
- Global Health Estimates 2019 Summary Tables: Deaths by Cause, Age and Sex, by World Bank Income Group, 2000-2019Document42 pagesGlobal Health Estimates 2019 Summary Tables: Deaths by Cause, Age and Sex, by World Bank Income Group, 2000-2019DanielaNo ratings yet
- To In-Vitro Antispasmodic Activity of Aqueous Leaves Extract of Coriandrum Sativum (C. Sativum) Linn. On Chicken IleumDocument5 pagesTo In-Vitro Antispasmodic Activity of Aqueous Leaves Extract of Coriandrum Sativum (C. Sativum) Linn. On Chicken IleumInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- RN MedSurgDocument685 pagesRN MedSurgArgyll Baye Ansuas100% (4)