You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Sample Journal Club 1Document2 pagesSample Journal Club 1aguocha1No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Indigo Children and AdultDocument5 pagesIndigo Children and AdultCristina-Maria Geambasu50% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Pharmacology of Analgesia and OpioidsDocument47 pagesPharmacology of Analgesia and Opioidsaguocha1No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Alchemy Heart Meditation C PDFDocument15 pagesAlchemy Heart Meditation C PDFaguocha1100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- What Is Microbial Ecology? What Is "Microbial"?Document34 pagesWhat Is Microbial Ecology? What Is "Microbial"?aguocha1No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Keys For Mastering Ascension - The Veca Consciousness CodesDocument26 pagesKeys For Mastering Ascension - The Veca Consciousness Codesaguocha198% (53)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Day 4 Gel ElectrophoresisDocument9 pagesDay 4 Gel Electrophoresisaguocha1No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- APBio Powerpointschm 1827Document126 pagesAPBio Powerpointschm 1827aguocha1No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Communication Skills For The Healthcare Professional - CDDocument268 pagesCommunication Skills For The Healthcare Professional - CDaguocha190% (10)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The AwakeningDocument128 pagesThe Awakeningaguocha1No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Stomach Cancer: The Ymptoms of Cancer AreDocument4 pagesStomach Cancer: The Ymptoms of Cancer Areaguocha1No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- In BetweenDocument4 pagesIn Betweenaguocha1No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Moment of Inertia Experiment 10 Physics 213 Hope Aguocha 12.11.14Document2 pagesMoment of Inertia Experiment 10 Physics 213 Hope Aguocha 12.11.14aguocha1No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Behavioral Neuroscience of TinnitudsDocument480 pagesThe Behavioral Neuroscience of TinnitudsBreiner Peñaranda100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Effects of Lyrical Music On Reading ComprehensionDocument14 pagesEffects of Lyrical Music On Reading ComprehensionIndik8No ratings yet
- Artificial Intelligence Unit 1 PPT Part 1Document81 pagesArtificial Intelligence Unit 1 PPT Part 1Imran SNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Chapter 1Document11 pagesChapter 1Jasie Joy GilloNo ratings yet
- Mental Health First AidDocument4 pagesMental Health First Aiddskubi8661No ratings yet
- Research Title ProposalDocument11 pagesResearch Title ProposalLiana BaluyotNo ratings yet
- An Investigation Into Student Teachers' Emotional Intelligence of Teaching Training Program: A Case Study at Loikaw..Document16 pagesAn Investigation Into Student Teachers' Emotional Intelligence of Teaching Training Program: A Case Study at Loikaw..Shreesh PatilNo ratings yet
- Técnicas de Visualização Criativa-EnDocument18 pagesTécnicas de Visualização Criativa-EnEmerson Juliano DiasNo ratings yet
- Physiology of Breathing and Respiratory Control During SleepDocument8 pagesPhysiology of Breathing and Respiratory Control During SleepAchmad Hafidz BaraqbahNo ratings yet
- Week 2 AssignmentDocument3 pagesWeek 2 AssignmentSolver TutorNo ratings yet
- Anatomy of Neuromuscular JunctionsDocument3 pagesAnatomy of Neuromuscular JunctionsValarmathiNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Exchange, Network, and Rational Choice TheoriesDocument11 pagesExchange, Network, and Rational Choice TheoriesVitas VitalyNo ratings yet
- Outdoor Plays Effect On Childhood DevelopmentDocument11 pagesOutdoor Plays Effect On Childhood DevelopmentRobert LavarnwayNo ratings yet
- Assignment 1. Mind MapDocument1 pageAssignment 1. Mind MapMaestros Plantel BayitoNo ratings yet
- Liebowitz Social Anxiety Scale (LSAS)Document2 pagesLiebowitz Social Anxiety Scale (LSAS)CC Britannia100% (1)
- The Neuroscience of Human Relationships: Attachment and The Developing Social Brain - Louis CozolinoDocument5 pagesThe Neuroscience of Human Relationships: Attachment and The Developing Social Brain - Louis Cozolinolewafofy67% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Anatomy and Physiology (Status Epilepticus)Document3 pagesAnatomy and Physiology (Status Epilepticus)Marvin John Labiano33% (3)
- Bigger Is Better: Primate Brain Size in Relationship To CognitionDocument19 pagesBigger Is Better: Primate Brain Size in Relationship To CognitionSANTIAGO VALENZUELA AMAYANo ratings yet
- Piaget - Resources PDFDocument4 pagesPiaget - Resources PDFapi-533984280No ratings yet
- Strategy Strand Focus Content Standard Learning Standard Integrated Learning Standard Objective Activities Materials ReflectionDocument4 pagesStrategy Strand Focus Content Standard Learning Standard Integrated Learning Standard Objective Activities Materials ReflectionJunior JR JNo ratings yet
- Appraisal ErrorsDocument15 pagesAppraisal ErrorsNaeem Khan100% (1)
- Social Influence and Its VarietiesDocument15 pagesSocial Influence and Its VarietiesYeda Cruz100% (1)
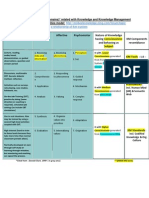
- Bloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Document1 pageBloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Md SantoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- UT Dallas Syllabus For cgs3342.501.10f Taught by Richard Golden (Golden)Document6 pagesUT Dallas Syllabus For cgs3342.501.10f Taught by Richard Golden (Golden)UT Dallas Provost's Technology GroupNo ratings yet
- Ankur Bhaumik 18895 UB201L Neurobiology Assignment Lab 1 and 2 PDFDocument4 pagesAnkur Bhaumik 18895 UB201L Neurobiology Assignment Lab 1 and 2 PDFAnkur BhaumikNo ratings yet
- Terminologia NeuroanatomicaDocument144 pagesTerminologia Neuroanatomicamatteo_vavassoriNo ratings yet
- Basic Elements of The Communication ProcessDocument13 pagesBasic Elements of The Communication ProcessMech JTubao67% (3)
- Neuro Quiz #1Document42 pagesNeuro Quiz #1Muhammad KaleemNo ratings yet
- The Benefits of HandsDocument2 pagesThe Benefits of HandsMark Anthony ORAANo ratings yet
- Information-Processing Theory - MED 7013 PDFDocument17 pagesInformation-Processing Theory - MED 7013 PDFhanaffi1No ratings yet