You might also like
- Example of Personal Development Plan SAMPLE ESSAYDocument8 pagesExample of Personal Development Plan SAMPLE ESSAYHanna LigyNo ratings yet
- 3.studi Kasus AsmaDocument2 pages3.studi Kasus AsmadelfiNo ratings yet
- THE INTERNATIONAL DRUG CONTROL SYSTEM, Adolphe Lande, 1974Document171 pagesTHE INTERNATIONAL DRUG CONTROL SYSTEM, Adolphe Lande, 1974Medicinal ColoradoNo ratings yet
- Slide 2 Principles of Interpersonal ComDocument16 pagesSlide 2 Principles of Interpersonal ComJean GanubNo ratings yet
- Self-Medication (PSBH Project 2010)Document54 pagesSelf-Medication (PSBH Project 2010)Varun Shah100% (1)
- Home Care Planning Guide SkilledDocument16 pagesHome Care Planning Guide SkilledswarnaNo ratings yet
- Managing Drug Suply ISTNDocument16 pagesManaging Drug Suply ISTNIndra PratamaNo ratings yet
- BS Industri Farmasi 2 2016-05-13 GP Farmasi Indonesia - Roadmap Industri Farmasi Nasional 2015-2025 RDDocument37 pagesBS Industri Farmasi 2 2016-05-13 GP Farmasi Indonesia - Roadmap Industri Farmasi Nasional 2015-2025 RDMas KulinNo ratings yet
- Weeek 1Document29 pagesWeeek 1Alvin De lunaNo ratings yet
- Presentasi Profil Industri FarmasiDocument105 pagesPresentasi Profil Industri FarmasiSyifaNurulAiniNo ratings yet
- Latest Amendment in Schedule YDocument30 pagesLatest Amendment in Schedule Yapi-384271179% (19)
- Prosiding Internasional Scopus MalaysiaDocument302 pagesProsiding Internasional Scopus MalaysiaSayati Mandia LubisNo ratings yet
- 9 Star PharmacistDocument4 pages9 Star PharmacistBenjel AndayaNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- Penggunaan Obat Herbal Pada Pasien Kanker ServiksDocument9 pagesPenggunaan Obat Herbal Pada Pasien Kanker ServiksislawatiNo ratings yet
- Tugas Jurnal Tentang Interaksi Dengan PelangganDocument14 pagesTugas Jurnal Tentang Interaksi Dengan PelangganTobiin HardirusitoNo ratings yet
- Evaluasi Kualitas Hidup Penderita Asma Di Kabupaten BelitungDocument8 pagesEvaluasi Kualitas Hidup Penderita Asma Di Kabupaten BelitungInanda DamantiaNo ratings yet
- 01 C & D Latar Belakang GPPDocument38 pages01 C & D Latar Belakang GPPPrisma TridaNo ratings yet
- Jurnal Polimer Fix PDFDocument5 pagesJurnal Polimer Fix PDFSherly Marcia DevanaNo ratings yet
- Case-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Document53 pagesCase-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Ditia RahimNo ratings yet
- Farmakoepidemiologi 2018 UmmDocument23 pagesFarmakoepidemiologi 2018 UmmSeptiani Ayu100% (1)
- Far Mako Eko NomiDocument59 pagesFar Mako Eko NomiLina LinuxNo ratings yet
- 44 85 1 SMDocument9 pages44 85 1 SMsilvanaanggraeniNo ratings yet
- Contoh Perhitungan QALYDocument6 pagesContoh Perhitungan QALYadrianne_apsNo ratings yet
- Pengembangan Biosimilar Indonesia - Sie Djohan (Kalbe Farma)Document55 pagesPengembangan Biosimilar Indonesia - Sie Djohan (Kalbe Farma)fathul jannah100% (2)
- Malaysia PRP Community Pharmacy LogbookDocument77 pagesMalaysia PRP Community Pharmacy LogbookAiWeiNo ratings yet
- Webinar Telefarmasi 25 Juli-DikonversiDocument30 pagesWebinar Telefarmasi 25 Juli-Dikonversiaqurniea qNo ratings yet
- (Radiant) RADVON PPT (161117) NardevDocument15 pages(Radiant) RADVON PPT (161117) NardevPradhipta WahyuNo ratings yet
- TDM Dan Rancangan Aturan DosisDocument37 pagesTDM Dan Rancangan Aturan Dosisadelin ransunNo ratings yet
- Drug Related ProblemDocument13 pagesDrug Related ProblemLinda Yuni LestariNo ratings yet
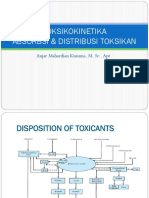
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieNo ratings yet
- Drug MGMTDocument138 pagesDrug MGMTShweelan Leon Sam100% (1)
- Usp 2020Document9 pagesUsp 2020titinrudyaniNo ratings yet
- Tinpus FarmakoekonomiDocument6 pagesTinpus FarmakoekonomiYesi Widya IswariNo ratings yet
- Studi Biofarmasi Obat Yang Diberikan Melalui MataDocument29 pagesStudi Biofarmasi Obat Yang Diberikan Melalui MataAry MaringNo ratings yet
- Jurnal Mohammad Anur Faiz 1508E006Document5 pagesJurnal Mohammad Anur Faiz 1508E006Yazta BintaraNo ratings yet
- Precede Proceed TM 8Document20 pagesPrecede Proceed TM 8MochamadAliHaidarNo ratings yet
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNo ratings yet
- Analisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangDocument12 pagesAnalisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangponekNo ratings yet
- Intropharma-MTM Core Elements 2Document24 pagesIntropharma-MTM Core Elements 2Marial PerlopNo ratings yet
- FARMAKOEKONOMI1Document38 pagesFARMAKOEKONOMI1AbnerDNeroNo ratings yet
- Drug Related Problem Dan SOAP WordDocument18 pagesDrug Related Problem Dan SOAP WordIflakhatul UlfaNo ratings yet
- Analisa Waktu Tunggu Pasien Terhadap Pelayanan Resep Rawat Jalan Di Apotik Puskesmas KotarajaDocument7 pagesAnalisa Waktu Tunggu Pasien Terhadap Pelayanan Resep Rawat Jalan Di Apotik Puskesmas KotarajaFara Ester100% (1)
- Drug Related ProblemsDocument40 pagesDrug Related Problemsfauzul husnaNo ratings yet
- Vaccine Development PowerPoint TemplatesDocument47 pagesVaccine Development PowerPoint TemplatesRizkiNo ratings yet
- Kinetik LengkapDocument133 pagesKinetik Lengkapreczky HasanNo ratings yet
- Pharmaceutical Care: by Musonda .K. Daka Department of Pharmacy School of Health Sciences University of ZambiaDocument20 pagesPharmaceutical Care: by Musonda .K. Daka Department of Pharmacy School of Health Sciences University of ZambiaLuka Mawele SinyangweNo ratings yet
- Brosur VialDocument2 pagesBrosur VialIndah Dwi PutriNo ratings yet
- Anti Protozoal AgentsDocument37 pagesAnti Protozoal AgentsGunjan YadavNo ratings yet
- Farmasi Rumah SakitDocument97 pagesFarmasi Rumah SakitkuronohanaNo ratings yet
- Pharmacokinetic Drug Interactions: Syed Imran Prof. Mrs. Vidya. P. SableDocument20 pagesPharmacokinetic Drug Interactions: Syed Imran Prof. Mrs. Vidya. P. SableDALI SAPARI 2021No ratings yet
- Asuhan Kefarmasian: Ahmad SalehDocument45 pagesAsuhan Kefarmasian: Ahmad SalehDjunaiddin FarmasiNo ratings yet
- Analisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanDocument14 pagesAnalisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanwahyuNo ratings yet
- Setiawan 2015Document8 pagesSetiawan 2015ShibaNo ratings yet
- Drug Utilization Study (Dus)Document17 pagesDrug Utilization Study (Dus)Arif Budiman100% (1)
- Farmakologi Pertemuan 6 ToksikologiDocument131 pagesFarmakologi Pertemuan 6 ToksikologiDeviati Juwita SariNo ratings yet
- CV Tri Murti AndayaniDocument7 pagesCV Tri Murti AndayaniAmalia UlfaNo ratings yet
- Systematic ReviewDocument13 pagesSystematic ReviewhsdgfjshdgfjshdgfNo ratings yet
- Managing Drug Suply 2017 KEDUADocument18 pagesManaging Drug Suply 2017 KEDUAwandameritaNo ratings yet
- MDS ProcurementDocument21 pagesMDS ProcurementSinthaNo ratings yet
- Real-World Evidence: How Big Data Is Changing Scientific StandardsDocument41 pagesReal-World Evidence: How Big Data Is Changing Scientific StandardsNational Press Foundation100% (3)
- Pharmaceuticals & Logistic Mechanisms, Grace Adeye (SPS)Document19 pagesPharmaceuticals & Logistic Mechanisms, Grace Adeye (SPS)Samuel MergaNo ratings yet
- Foodborne DiseaseDocument12 pagesFoodborne DiseasewandameritaNo ratings yet
- Managing Drug Suply 2017 KEDUADocument18 pagesManaging Drug Suply 2017 KEDUAwandameritaNo ratings yet
- Food and Toxicity-Natural ToxinsDocument47 pagesFood and Toxicity-Natural Toxinswandamerita100% (1)
- Jurnal Sirsak PDFDocument5 pagesJurnal Sirsak PDFwandameritaNo ratings yet
- Modul4 CRT SPT SystDocument22 pagesModul4 CRT SPT SystwandameritaNo ratings yet
- Pharmacy Manager Pharmacist in Charge Healthcare in New York NY Resume Trupti GandhiDocument2 pagesPharmacy Manager Pharmacist in Charge Healthcare in New York NY Resume Trupti GandhiTruptiGandhiNo ratings yet
- Ahimajournal 2014 10 DLDocument101 pagesAhimajournal 2014 10 DLDarrin OpdyckeNo ratings yet
- Bozeman Deaconess Proposal For Big Sky HospitalDocument48 pagesBozeman Deaconess Proposal For Big Sky HospitalBozeman Daily ChronicleNo ratings yet
- ReferatDocument23 pagesReferatmirantikaNo ratings yet
- QPP COVID-19 Response Fact SheetDocument14 pagesQPP COVID-19 Response Fact SheetWaseemNo ratings yet
- Manual For Medicines Good DispensingDocument114 pagesManual For Medicines Good DispensingJosh SorianoNo ratings yet
- MGT-341 Disaster Preparedness For Hospitals and Healthcare OrganizationsDocument2 pagesMGT-341 Disaster Preparedness For Hospitals and Healthcare OrganizationsbillcotterNo ratings yet
- Spravato Sample Exception LetterDocument1 pageSpravato Sample Exception LetterspamcastNo ratings yet
- Letters For Issue On 19.07.2011: 1. Be Noc/Test LicenceDocument9 pagesLetters For Issue On 19.07.2011: 1. Be Noc/Test LicenceTanuj VarshneyNo ratings yet
- 420 Poster PotxDocument1 page420 Poster Potxapi-355200259No ratings yet
- Rcog PretermDocument13 pagesRcog Pretermsintiadamayanti100% (1)
- Allergy 2010Document7 pagesAllergy 2010HAOMSNo ratings yet
- Joan Tortorici, RN, BSN Recognized As A Professional of The Year by Strathmore's Who's Who Worldwide PublicationDocument2 pagesJoan Tortorici, RN, BSN Recognized As A Professional of The Year by Strathmore's Who's Who Worldwide PublicationPR.comNo ratings yet
- Sample Persuasive Policy SpeechesDocument12 pagesSample Persuasive Policy Speechescyspace100% (1)
- CAP Checklist 110718Document53 pagesCAP Checklist 110718yousrazeidan1979No ratings yet
- Fund For Hope Application 2019Document1 pageFund For Hope Application 2019Jesus BergNo ratings yet
- The The Practice of Clinical Neuropsychology Studies On Neuropsychology Development and CognitionDocument392 pagesThe The Practice of Clinical Neuropsychology Studies On Neuropsychology Development and CognitionJelena Jovanovic100% (6)
- RadNet Investor PresentationDocument23 pagesRadNet Investor PresentationtheredcornerNo ratings yet
- ORNAP 35th Annual Convention and Scientific MeetingDocument2 pagesORNAP 35th Annual Convention and Scientific MeetingNURSES' PADNo ratings yet
- Hammer Map Kpis Hfma NJ 11 Jan 2011Document182 pagesHammer Map Kpis Hfma NJ 11 Jan 2011maryannalbert100% (1)
- The Modified Caregiver Strain Index (CSI)Document2 pagesThe Modified Caregiver Strain Index (CSI)dvr_donNo ratings yet
- Community Medicine 2012-2013Document9 pagesCommunity Medicine 2012-2013Aftab AhmadNo ratings yet
- Michigan Medicaid Claim Predictive Modeling PolicyDocument2 pagesMichigan Medicaid Claim Predictive Modeling PolicyBeverly TranNo ratings yet
- TCS India FAQs - Pharmacy BenefitsDocument9 pagesTCS India FAQs - Pharmacy BenefitsabhilashNo ratings yet
- Fact Sheet FinalDocument2 pagesFact Sheet FinalevangelinaNo ratings yet
- Health Management Information Systems: Computerized Provider Order Entry (CPOE) Lecture BDocument18 pagesHealth Management Information Systems: Computerized Provider Order Entry (CPOE) Lecture BHealth IT Workforce Curriculum - 2012No ratings yet
- Journal Nursing DocumentationDocument8 pagesJournal Nursing DocumentationikaNo ratings yet
- Resep (Disalin Sesuai Aslinya) Drug Related Problem (S) : Kertas Kerja Tinjauan Dan Pelayanan ResepDocument3 pagesResep (Disalin Sesuai Aslinya) Drug Related Problem (S) : Kertas Kerja Tinjauan Dan Pelayanan ResepHerlina AlfianyNo ratings yet