You might also like
- Multiple TraumaDocument78 pagesMultiple Traumasgod34No ratings yet
- Antibiotic Prophylaxis in Open Fractures GuidelineDocument2 pagesAntibiotic Prophylaxis in Open Fractures GuidelineubayyumrNo ratings yet
- Acute Coronary Syndrome: Mini LectureDocument16 pagesAcute Coronary Syndrome: Mini LectureMaRc RaFfy BauTista FeliciaNoNo ratings yet
- Guideline HF 2013Document79 pagesGuideline HF 2013supit1No ratings yet
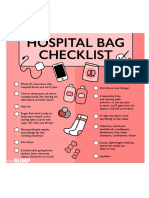
- Hospital Bag ChecklistDocument2 pagesHospital Bag ChecklistikhwanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CHCICS305A Provide Behaviour Support in The Context of Individualised PlansDocument100 pagesCHCICS305A Provide Behaviour Support in The Context of Individualised PlansBhakta Chand ThakuriNo ratings yet
- Interprofessional Collaboration IDocument10 pagesInterprofessional Collaboration IRia Qadariah AriefNo ratings yet
- ACOSDocument14 pagesACOSDejan ŽujovićNo ratings yet
- Plete Angelinesimulation Assignment ActivityDocument2 pagesPlete Angelinesimulation Assignment ActivityRoel John Atamosa CasilacNo ratings yet
- Common Psychiatric Symptoms and Key Terms in Psychiatric NursingDocument3 pagesCommon Psychiatric Symptoms and Key Terms in Psychiatric NursingQueeny Anne ApilNo ratings yet
- Friday Problem Statement PresentationDocument7 pagesFriday Problem Statement PresentationyashramawatNo ratings yet
- Guide To Interpreting MicsDocument4 pagesGuide To Interpreting MicsVlad VladNo ratings yet
- Teaching Philosophy Assignment Patricia AnyasoDocument6 pagesTeaching Philosophy Assignment Patricia Anyasoodunze1No ratings yet
- Capitol University: College of Nursing Cagayan de Oro CityDocument2 pagesCapitol University: College of Nursing Cagayan de Oro CityChaine Agolito100% (1)
- Pe1 Lesson 4 Cardiorespiratory and Muskuloskeletal FitnessDocument53 pagesPe1 Lesson 4 Cardiorespiratory and Muskuloskeletal Fitnessdario serranoNo ratings yet
- Voh 11Document19 pagesVoh 11Siphiwe Christopher MathebulaNo ratings yet
- Tips To Improve MemoryDocument4 pagesTips To Improve Memoryoscar gmNo ratings yet
- Apollo Case AnalysisDocument8 pagesApollo Case AnalysismuddanapNo ratings yet
- Teacher StressDocument9 pagesTeacher StressHanah FernandezNo ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (B)Document19 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (B)Nashebah A. BatuganNo ratings yet
- Lesson 1: Personal Physical Activity InventoryDocument10 pagesLesson 1: Personal Physical Activity InventoryCharmaine JanorasNo ratings yet
- Neonatal MortalityDocument8 pagesNeonatal MortalityGlady Jane TevesNo ratings yet
- Barriers To Health Technology AssessmentDocument8 pagesBarriers To Health Technology AssessmentHilton D. CalawenNo ratings yet
- Is Technology Isolating UsDocument2 pagesIs Technology Isolating UsJOANA LLANANo ratings yet
- PICOT QuestionDocument1 pagePICOT Questionmelodia gandezaNo ratings yet
- Assessment Questions (Assessment Criteria)Document2 pagesAssessment Questions (Assessment Criteria)sujanaNo ratings yet
- Abstract Comparison Between Albendazole and MebendazoleDocument25 pagesAbstract Comparison Between Albendazole and MebendazoleluzNo ratings yet
- Child With Unsteady GaitDocument2 pagesChild With Unsteady GaitAya MahmoudNo ratings yet
- PH Di TMDUDocument7 pagesPH Di TMDUFariz NurwidyaNo ratings yet
- Intro Quiz - 2.14.23Document3 pagesIntro Quiz - 2.14.23Casey Alyssa Therese CaayamanNo ratings yet
- Cyclosporine PharmaDocument2 pagesCyclosporine PharmaflagaacNo ratings yet
- An Evidence Based Case Study To Identify The Role of Bothrops Lanceolatus As A Homeopathic AnticoagulantDocument6 pagesAn Evidence Based Case Study To Identify The Role of Bothrops Lanceolatus As A Homeopathic AnticoagulantEditor IJTSRDNo ratings yet
- Trends in Midwifry and ObstetricsDocument8 pagesTrends in Midwifry and ObstetricsVarna MohanNo ratings yet
- Notes:: Sons Lives AwayDocument4 pagesNotes:: Sons Lives Awaykuriakose mathewNo ratings yet
- David Fetterer ResumeDocument3 pagesDavid Fetterer ResumedfettererNo ratings yet