You might also like
- EKG Nclex High YieldDocument13 pagesEKG Nclex High Yieldnene lewis100% (1)
- Cardiovascular System: By: S@JDocument35 pagesCardiovascular System: By: S@JD TekNo ratings yet
- Rheumatic FeverDocument87 pagesRheumatic FeverFarida Mawaddah Husna100% (1)
- Cardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNDocument49 pagesCardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNrosieglaeNo ratings yet
- Treatment of Resistant and Refractory HypertensionDocument21 pagesTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- DRIPSDocument7 pagesDRIPSKim Alvarez100% (2)
- MyocarditisDocument29 pagesMyocarditishastonniiNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Heart SoundsDocument4 pagesHeart SoundsAthieNo ratings yet
- Cerebrovascular Accident (CVA)Document71 pagesCerebrovascular Accident (CVA)nur muizzah afifah hussinNo ratings yet
- Diabetic Neuropathy PPT Final2Document61 pagesDiabetic Neuropathy PPT Final2Jenny Juniora Ajoc100% (1)
- ACLS Answer KeyDocument23 pagesACLS Answer KeyKirana Budhiarta94% (17)
- Cardiovascular Examination:: General InspectionDocument6 pagesCardiovascular Examination:: General InspectionPhysician AssociateNo ratings yet
- Soap NotesDocument3 pagesSoap Notesapi-383904539No ratings yet
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 pagesFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949No ratings yet
- Congenital Heart Disease - Cynotic AcynoticDocument34 pagesCongenital Heart Disease - Cynotic Acynoticvruttika parmarNo ratings yet
- ASTHMADocument82 pagesASTHMAImmanuel100% (1)
- Acute Coronary Syndrome: Dr. H.M. Saifullah Napu, SPJP, FihaDocument47 pagesAcute Coronary Syndrome: Dr. H.M. Saifullah Napu, SPJP, FihaJual Beli Promosi100% (1)
- Managing Psychiatric Patients in The EDDocument28 pagesManaging Psychiatric Patients in The EDfadiNo ratings yet
- Heart Failure in ChildrenDocument44 pagesHeart Failure in ChildrenRisna Ariani100% (2)
- Chapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureDocument15 pagesChapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureWorrawalun FuktongNo ratings yet
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Document46 pagesPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- What Is HyperlipidemiaDocument9 pagesWhat Is Hyperlipidemiaichanara100% (2)
- PericarditisDocument29 pagesPericarditisPavin KumarNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Nephrotic Syndrome in Children: January 2013Document7 pagesNephrotic Syndrome in Children: January 2013molenNo ratings yet
- Pathophysiology of Arrhythmias: Belay E. MD December 2015Document53 pagesPathophysiology of Arrhythmias: Belay E. MD December 2015Amanuel MaruNo ratings yet
- Surgical Treatment For BREAST CANCERDocument5 pagesSurgical Treatment For BREAST CANCERJericho James TopacioNo ratings yet
- Abdominal TuberculosisDocument36 pagesAbdominal TuberculosisImmanuel50% (2)
- Diabetes Case StudyDocument9 pagesDiabetes Case StudyFajri Nur PrasetyoNo ratings yet
- Cardinal Manifestations of Neurologic DiseaseDocument79 pagesCardinal Manifestations of Neurologic DiseaseImmanuel100% (2)
- Pediatric Cardiovascular DiseasesDocument4 pagesPediatric Cardiovascular DiseasesWendy EscalanteNo ratings yet
- Blood TransfusionDocument14 pagesBlood TransfusionSarah Uy CaronanNo ratings yet
- Bronchiectasis OkDocument60 pagesBronchiectasis OkImmanuelNo ratings yet
- BRONCHIECTASISDocument40 pagesBRONCHIECTASISImmanuel100% (2)
- PericarditisDocument4 pagesPericarditisGeorge Chaucer HwangNo ratings yet
- Dissiminated Intravascular Coagulation PathoDocument2 pagesDissiminated Intravascular Coagulation Pathoapi-341263362No ratings yet
- Understanding Low Blood Pressure - The BasicsDocument6 pagesUnderstanding Low Blood Pressure - The BasicsRajeev Nechiyil100% (1)
- Cardiomyopathy and MyocarditisDocument8 pagesCardiomyopathy and Myocarditisoddone_out100% (1)
- Abruptio PlacentaeDocument4 pagesAbruptio PlacentaeMelissa Aina Mohd YusofNo ratings yet
- Coarctation of The AortaDocument15 pagesCoarctation of The AortaNadiyaSiddiquiNo ratings yet
- Prevention of CancerDocument2 pagesPrevention of Cancercmmc_3No ratings yet
- Reye's SyndromeDocument11 pagesReye's SyndromeChristine Go100% (1)
- Case 36 AscitesDocument4 pagesCase 36 AscitesMichaelNo ratings yet
- Med Surg MidtermDocument17 pagesMed Surg Midtermjhan grabierNo ratings yet
- Hypertension NotesDocument7 pagesHypertension Notesapi-3697326100% (3)
- Cardiac (Heart) FailureDocument27 pagesCardiac (Heart) FailureSanthoshi Sadhanaa SankarNo ratings yet
- Supine Hypotensive SyndromeDocument6 pagesSupine Hypotensive SyndromeDimas RadityaNo ratings yet
- Tropical Splenomegaly SyndromeDocument12 pagesTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Peds Lecture 3Document19 pagesPeds Lecture 3Suraj Mukatira100% (1)
- IntubationDocument70 pagesIntubationkatnev100% (1)
- Prepared by Mary Ann A. Cubon, RN, RM, ManDocument35 pagesPrepared by Mary Ann A. Cubon, RN, RM, ManCarlaLuisaVillalunaNo ratings yet
- 1538 Exam 4 Cell Reg & GriefDocument35 pages1538 Exam 4 Cell Reg & GriefJade EdanoNo ratings yet
- Coarctation of AortaDocument11 pagesCoarctation of AortaThe Medical PostNo ratings yet
- Gastro MnemonicsDocument8 pagesGastro MnemonicsRufina SoomroNo ratings yet
- Nurs Pocket CardsDocument10 pagesNurs Pocket CardsKiara SalvageNo ratings yet
- Bronchial AsthmaDocument27 pagesBronchial AsthmachandrikaismailNo ratings yet
- Gestational DiabetesDocument51 pagesGestational Diabeteskhadzx100% (2)
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Sudden Infant Death Syndrome and The Child Care ProfessionDocument36 pagesSudden Infant Death Syndrome and The Child Care ProfessionIsos CellNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- SOAP NotesDocument4 pagesSOAP Notesemmag79No ratings yet
- Emergency MnemonicDocument5 pagesEmergency Mnemonicanon_549623261No ratings yet
- Pediatrics Notes: ND STDocument20 pagesPediatrics Notes: ND STsatriobudi_wicaksonoNo ratings yet
- Heart Failure CaseDocument2 pagesHeart Failure CasePaulo Arwin BaduriaNo ratings yet
- Heart Failure and CAD Case StudyDocument38 pagesHeart Failure and CAD Case StudyAbno NavarreteNo ratings yet
- Pathophysiology of AF in CHFDocument5 pagesPathophysiology of AF in CHFBimaIndraNo ratings yet
- Cardiac CatheterizationDocument2 pagesCardiac Catheterizationjacallis50% (2)
- Notes For Clincal CasesDocument12 pagesNotes For Clincal CasesMandeepNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Testing Documents v1.1Document1 pageTesting Documents v1.1ImmanuelNo ratings yet
- Cholera ARDocument6 pagesCholera ARImmanuelNo ratings yet
- Testing Documents v1.1Document1 pageTesting Documents v1.1ImmanuelNo ratings yet
- Cholera DKLDocument59 pagesCholera DKLImmanuel100% (1)
- Cardiomyopathy and MyocarditisDocument69 pagesCardiomyopathy and MyocarditisImmanuel100% (1)
- Cerebral Palsydkl 5Document22 pagesCerebral Palsydkl 5ImmanuelNo ratings yet
- What Is Cardiomyopathy?Document11 pagesWhat Is Cardiomyopathy?ImmanuelNo ratings yet
- Case of COPDDocument1 pageCase of COPDImmanuelNo ratings yet
- Acute Inflammatory Demyelinating PolyneuropathyDocument55 pagesAcute Inflammatory Demyelinating PolyneuropathyImmanuel100% (1)
- Cardiac Arrest and CPR ARDocument11 pagesCardiac Arrest and CPR ARImmanuelNo ratings yet
- CancerDocument109 pagesCancerImmanuelNo ratings yet
- Abdominal TuberculosisDocument9 pagesAbdominal TuberculosisImmanuelNo ratings yet
- Abnoramal ECGDocument20 pagesAbnoramal ECGImmanuelNo ratings yet
- Abdominal tuberculosis 修Document47 pagesAbdominal tuberculosis 修ImmanuelNo ratings yet
- Code of Ethics 2017Document74 pagesCode of Ethics 2017ImmanuelNo ratings yet
- Heart Diseases in PregnancyDocument19 pagesHeart Diseases in PregnancyKirubah Sai PatnaikNo ratings yet
- Ecg Short AnswerDocument3 pagesEcg Short AnswerZoey SanNo ratings yet
- Esc Guidelines 2020 Nste-Acs FinalDocument34 pagesEsc Guidelines 2020 Nste-Acs FinalabcdefNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- Left Anterior Fascicular Block (LAFB) ECG Review - Criteria and ExamplesDocument1 pageLeft Anterior Fascicular Block (LAFB) ECG Review - Criteria and ExamplesWiwik Puji LestariNo ratings yet
- Gallop RhythmDocument2 pagesGallop RhythmMuhammad SulamanNo ratings yet
- Wolff Parkinson White SyndromeDocument3 pagesWolff Parkinson White SyndromeYong Fang YueNo ratings yet
- Prevalensi Atrioventrikular Blok Di RSUP Prof. Dr. R. D. Kandou Manado Periode 2013 - 2014Document6 pagesPrevalensi Atrioventrikular Blok Di RSUP Prof. Dr. R. D. Kandou Manado Periode 2013 - 2014Herlinda Puji LNo ratings yet
- AmiodaroneDocument2 pagesAmiodaroneEmmil BernardoNo ratings yet
- Myocardial Infarction: Classification of ACSDocument7 pagesMyocardial Infarction: Classification of ACSMaria Charis Anne IndananNo ratings yet
- EkgppDocument93 pagesEkgppLindsay WishmierNo ratings yet
- Cardiac CycleDocument14 pagesCardiac Cycleareznik3007No ratings yet
- Abnormal EcgDocument6 pagesAbnormal EcgYash Raj SisodiyaNo ratings yet
- Ebook Current Diagnosis and Treatment Cardiology 5Th Edition PDF Full Chapter PDFDocument67 pagesEbook Current Diagnosis and Treatment Cardiology 5Th Edition PDF Full Chapter PDFbeth.hao417100% (31)
- Rigel Uni Sim Lite DatasheetDocument5 pagesRigel Uni Sim Lite Datasheetmailalexmd.vrn.ruNo ratings yet
- Mitral Valve Prolapse (MVP) : Auscultation of MurmursDocument55 pagesMitral Valve Prolapse (MVP) : Auscultation of MurmursYagyeshNo ratings yet
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
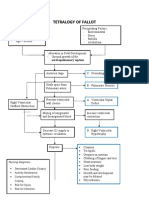
- Concept Map Tetralogy of FallotDocument2 pagesConcept Map Tetralogy of FallotKarl KiwisNo ratings yet
- Atlas of ECGDocument162 pagesAtlas of ECGMiuschaNo ratings yet
- Bifascicular Block Revealing Steinerts Myotonic DystrophyDocument8 pagesBifascicular Block Revealing Steinerts Myotonic DystrophyIJAR JOURNALNo ratings yet
- Glasgow PhysiciansGuideDocument90 pagesGlasgow PhysiciansGuideIstván Kecskés100% (1)
- Diagnostic Pacing Maneuvers Part 1Document16 pagesDiagnostic Pacing Maneuvers Part 1chirudarsiNo ratings yet