You might also like
- Tumor Thrombus: Incidence, Imaging, Prognosis and TreatmentDocument13 pagesTumor Thrombus: Incidence, Imaging, Prognosis and TreatmentDuccio RossiNo ratings yet
- Renal Cell Carcinoma Surgical Treatment: DR Bilal Ahmad Resident Surgeon Urology BBH RawalpindiDocument38 pagesRenal Cell Carcinoma Surgical Treatment: DR Bilal Ahmad Resident Surgeon Urology BBH Rawalpindiumair ahmadNo ratings yet
- Sakamoto 2017Document6 pagesSakamoto 2017Chris WuNo ratings yet
- Obstructive Jaundice: Dr. SrinivasDocument52 pagesObstructive Jaundice: Dr. SrinivasSahir100% (1)
- MNGT of Renal Tumors-2Document66 pagesMNGT of Renal Tumors-2Tsega WesenNo ratings yet
- Renal CancerDocument13 pagesRenal CancerDavid RyanNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Carcinoma CervixDocument45 pagesCarcinoma CervixDhananjaya ShivalingappaNo ratings yet
- Surgery III MCQS 2023Document4 pagesSurgery III MCQS 2023mariamNo ratings yet
- (Onco) Oncologic EmergenciesDocument71 pages(Onco) Oncologic EmergencieshatsuneNo ratings yet
- Cholangiocarcinoma: R.KarthikeyanDocument49 pagesCholangiocarcinoma: R.KarthikeyanKarthikeyan R100% (2)
- Surgery MrcsDocument339 pagesSurgery Mrcsdr_shafiq80% (10)
- SurgeryDocument30 pagesSurgeryLuai Tuma KhouryNo ratings yet
- Colorectal Ca (CRC) .: Malueth Abraham, MBCHB ViDocument36 pagesColorectal Ca (CRC) .: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- EAU Pocket On Renal Cell Carcinoma 2022Document28 pagesEAU Pocket On Renal Cell Carcinoma 2022Dane QhNo ratings yet
- Surgery III 2023 EXAMDocument5 pagesSurgery III 2023 EXAMmariamNo ratings yet
- Jordanian Surgical Society - PPT LastDocument166 pagesJordanian Surgical Society - PPT LastNessreen Jamal100% (1)
- Colorectal CancersDocument162 pagesColorectal CancersSomto NwabuezeNo ratings yet
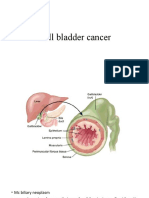
- CA Gall BladderDocument24 pagesCA Gall BladderTheoder RobinsonNo ratings yet
- Cardiothoracics ReviewDocument44 pagesCardiothoracics ReviewGrace LNo ratings yet
- Carcinoma of Renal Pelvis and UreterDocument27 pagesCarcinoma of Renal Pelvis and UreterIsaac MwangiNo ratings yet
- Role of Lymphadenectomy in Genitourinary MalignanciesDocument5 pagesRole of Lymphadenectomy in Genitourinary Malignanciesmohammed hassonaNo ratings yet
- Surgery Bladder TumorDocument35 pagesSurgery Bladder TumorMuhammad ArsalNo ratings yet
- Gall Bladder CancerDocument29 pagesGall Bladder CancerJoju SebastianNo ratings yet
- Colon and Rectal CancerDocument62 pagesColon and Rectal CancerSK TalkNo ratings yet
- Oleh: DR - Hans Marpaung, SPB, FicsDocument75 pagesOleh: DR - Hans Marpaung, SPB, FicsIrma Julyanti PanggabeanNo ratings yet
- AFIU Post Op Managment of Renal Transplant - Prof Saeed AkhtarDocument55 pagesAFIU Post Op Managment of Renal Transplant - Prof Saeed AkhtarUmar FarooqNo ratings yet
- Common Bile Duct Stones StrictureDocument48 pagesCommon Bile Duct Stones StrictureSyarif MalawatNo ratings yet
- Esophageal Carcinoma: Mark Louie M. Lanting, MDDocument44 pagesEsophageal Carcinoma: Mark Louie M. Lanting, MDlouie10279098No ratings yet
- Article File For CsiiDocument3 pagesArticle File For Csiiapi-205989841No ratings yet
- Management of Lung Cancer by DR Abdul-AzizDocument89 pagesManagement of Lung Cancer by DR Abdul-AzizAbdulaziz HassenNo ratings yet
- Biliary Tract Cancer: Presented By: DR Ankit Lalchandani Moderated By: DR MP SinghDocument36 pagesBiliary Tract Cancer: Presented By: DR Ankit Lalchandani Moderated By: DR MP SinghAnkit LalchandaniNo ratings yet
- Urinary Bladder and Renal Cell CarcinomaDocument21 pagesUrinary Bladder and Renal Cell CarcinomaYazeed AsrawiNo ratings yet
- PICC Line DVTDocument9 pagesPICC Line DVTAnonymous ZUaUz1wwNo ratings yet
- Advances in Surgery-LrrcDocument62 pagesAdvances in Surgery-LrrcHarshit SrivastavaNo ratings yet
- CoronarografieDocument72 pagesCoronarografieLaurentiu AndreiNo ratings yet
- Catheter-Related Thrombosis - A Practical Approach - PMCDocument14 pagesCatheter-Related Thrombosis - A Practical Approach - PMCRejo JohnNo ratings yet
- Thoracic and Abdominal TraumaDocument76 pagesThoracic and Abdominal Traumajhk0428100% (1)
- Respiration 11 Bronchogenic CarcinomaDocument48 pagesRespiration 11 Bronchogenic Carcinomaapi-19641337No ratings yet
- Radical Surgery For Cancer of The Pancreas: Kothaj PDocument3 pagesRadical Surgery For Cancer of The Pancreas: Kothaj Pyacine26No ratings yet
- Transplant Liver Imaging PresentationDocument48 pagesTransplant Liver Imaging PresentationChristopher MejiasNo ratings yet
- Pra VeenDocument88 pagesPra VeenPraveen PraviiNo ratings yet
- EAU Pocket On Renal Cell Carcinoma 2023Document29 pagesEAU Pocket On Renal Cell Carcinoma 2023Phuoc LeNo ratings yet
- AsdfsadafsdDocument369 pagesAsdfsadafsdfrankmalcovNo ratings yet
- Hilar Cholangiocarcinoma: Therapeutic Strategies: MT KhalfallahDocument49 pagesHilar Cholangiocarcinoma: Therapeutic Strategies: MT KhalfallahKhalfallah Mohamed TaharNo ratings yet
- Pancreatic Cancer: Dr. Tjatur Winarsanto SPPDDocument41 pagesPancreatic Cancer: Dr. Tjatur Winarsanto SPPDMayiz Renata LimerseNo ratings yet
- CarcinomarectumDocument45 pagesCarcinomarectumHuzefa MemonNo ratings yet
- EAU Pocket On Renal Cell Carcinoma 2024Document35 pagesEAU Pocket On Renal Cell Carcinoma 2024nadaelhaousNo ratings yet
- Neoplasms of The Genitourinary TractDocument71 pagesNeoplasms of The Genitourinary Tractvishalzenia100% (2)
- Cardiac Surgery Coronary I e IIDocument43 pagesCardiac Surgery Coronary I e IIFrancisNo ratings yet
- Rectal Ca:: Malueth Abraham, MBCHB ViDocument32 pagesRectal Ca:: Malueth Abraham, MBCHB ViMalueth AnguiNo ratings yet
- Cancer NotesDocument12 pagesCancer Noteswavezone113No ratings yet
- Friedman RadiologiDocument20 pagesFriedman RadiologiVela NazarNo ratings yet
- Neoplasms of Kidney and BladderDocument51 pagesNeoplasms of Kidney and BladderSK TalkNo ratings yet
- Hilar Cholangiocarcinoma Diagnosed and Treated Early, in Prejaundice PhaseDocument4 pagesHilar Cholangiocarcinoma Diagnosed and Treated Early, in Prejaundice PhasebbdddNo ratings yet
- Lower Gi Bleed 4611Document23 pagesLower Gi Bleed 4611Mien BuntaraNo ratings yet
- Endovascular InterventionsFrom EverandEndovascular InterventionsJose M. WileyNo ratings yet
- Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and ManagementFrom EverandPancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and ManagementNo ratings yet
- Colorectal Surgery: Clinical Care and ManagementFrom EverandColorectal Surgery: Clinical Care and ManagementBruce GeorgeNo ratings yet
- PR Kateterisasi Pada TbiDocument8 pagesPR Kateterisasi Pada TbiAgung IndraNo ratings yet
- Suture Material: Mangkubumi Putra WijayaDocument37 pagesSuture Material: Mangkubumi Putra WijayaAgung IndraNo ratings yet
- SirkumDocument22 pagesSirkumAgung IndraNo ratings yet
- Presentation 1Document14 pagesPresentation 1Agung IndraNo ratings yet
- Urothelial Tumors of The Upper Urinary Tract FixDocument25 pagesUrothelial Tumors of The Upper Urinary Tract FixAgung IndraNo ratings yet
- PR NHL Dan HerniaDocument23 pagesPR NHL Dan HerniaAgung IndraNo ratings yet
- Guildeline CA Penis KemoterapiDocument18 pagesGuildeline CA Penis KemoterapiAgung IndraNo ratings yet
- Wound CareDocument13 pagesWound CareAgung IndraNo ratings yet
- Meatotomy and Wound CareDocument13 pagesMeatotomy and Wound CareAgung IndraNo ratings yet
- PR Kateterisasi Pada TbiDocument8 pagesPR Kateterisasi Pada TbiAgung IndraNo ratings yet
- The Use of Medical Expulsive Therapy During Pregnancy: A Worldwide Perspective Among ExpertsDocument18 pagesThe Use of Medical Expulsive Therapy During Pregnancy: A Worldwide Perspective Among ExpertsAgung IndraNo ratings yet
- Deep Vein Thrombosis: Faculty of Medicine University of BrawijayaDocument59 pagesDeep Vein Thrombosis: Faculty of Medicine University of BrawijayaAgung IndraNo ratings yet
- MeatotomyDocument11 pagesMeatotomyAgung Indra100% (1)
- Orchidoscopy Journal Fix 2Document24 pagesOrchidoscopy Journal Fix 2Agung IndraNo ratings yet
- PujoDocument4 pagesPujoAgung IndraNo ratings yet
- AirwayTrauma FullRepDocument62 pagesAirwayTrauma FullRepMuhammad Agung WNo ratings yet
- Pap Smear Technique: VideoDocument15 pagesPap Smear Technique: VideoYuskamita KarsaeniNo ratings yet
- Jornal Reading Understanding The Ureter FixDocument25 pagesJornal Reading Understanding The Ureter FixAgung IndraNo ratings yet
- Case PresentationDocument13 pagesCase PresentationAgung IndraNo ratings yet
- A Worldwide Perspective Among ExpertsDocument17 pagesA Worldwide Perspective Among ExpertsAgung IndraNo ratings yet
- Abd Trauma - Cindy KinDocument27 pagesAbd Trauma - Cindy KinAgung IndraNo ratings yet
- Cardiogenic ShockDocument40 pagesCardiogenic ShockAgung IndraNo ratings yet
- Orchidoscopy Journal FixDocument23 pagesOrchidoscopy Journal FixAgung IndraNo ratings yet
- Guildeline CA Penis KemoterapiDocument18 pagesGuildeline CA Penis KemoterapiAgung IndraNo ratings yet
- Expert Lecture (Bleeding Disorders)Document24 pagesExpert Lecture (Bleeding Disorders)Agung IndraNo ratings yet
- Hasil Lab (18/6) Rentang Normal Rentang Normal Hematologi UrinalisisDocument1 pageHasil Lab (18/6) Rentang Normal Rentang Normal Hematologi UrinalisisAgung IndraNo ratings yet
- Deep Vein Thrombosis: Faculty of Medicine University of BrawijayaDocument59 pagesDeep Vein Thrombosis: Faculty of Medicine University of BrawijayaAgung IndraNo ratings yet
- Cardiovascular System: by M. Rasjad IndraDocument14 pagesCardiovascular System: by M. Rasjad IndraAgung IndraNo ratings yet
- Proses Diagnostik - KuliahDocument52 pagesProses Diagnostik - KuliahAgung Indra100% (1)
- Use of Simulation Based Medical Education For AdvaDocument4 pagesUse of Simulation Based Medical Education For AdvaLê Huy HoàngNo ratings yet
- Poor and Rich CountriesDocument5 pagesPoor and Rich Countriestwentyeight28No ratings yet
- Poet Report: KRAS Testing For Colorectal CancerDocument9 pagesPoet Report: KRAS Testing For Colorectal CancerJohn KentNo ratings yet
- Sample Discharge SummaryDocument4 pagesSample Discharge SummaryPatient Safety My100% (2)
- Interprofessional Education DR DianthaDocument24 pagesInterprofessional Education DR DianthaInges PSNo ratings yet
- A Psychometric Evaluation of The Personality Assessment Inventory - Short Form Clinical Scales in An Inpatient Psychiatric SampleDocument5 pagesA Psychometric Evaluation of The Personality Assessment Inventory - Short Form Clinical Scales in An Inpatient Psychiatric SampleLuís Costa da SilvaNo ratings yet
- ALT Practical Handout For 2nd Year MBBSDocument4 pagesALT Practical Handout For 2nd Year MBBSfreddy fitriadyNo ratings yet
- Avian Nutrition Tube Feeding BirdsDocument5 pagesAvian Nutrition Tube Feeding BirdsLe KhaiNo ratings yet
- Identification and Classification of Neonate With InfectionsDocument62 pagesIdentification and Classification of Neonate With Infectionsvisuinsvu100% (7)
- Nursing Care of The Patient With Neurological DisordersDocument89 pagesNursing Care of The Patient With Neurological DisordersShara Mae More BarriosNo ratings yet
- Cis Self-Study Lesson Plan: Instruments For Total Knee ArthroplastyDocument3 pagesCis Self-Study Lesson Plan: Instruments For Total Knee Arthroplastyjerimiah_manzonNo ratings yet
- Managemnet Arterial UlcersDocument24 pagesManagemnet Arterial UlcersMohamad Zulfikar100% (1)
- PNFDocument13 pagesPNFMohd Murtadha Ramly100% (1)
- (NCPS) Impaired Physical Mobility 2Document2 pages(NCPS) Impaired Physical Mobility 2roren100% (1)
- ADC Exam - MCQDocument10 pagesADC Exam - MCQHatem Abouelnasr100% (10)
- Ethics Test Bank ch3Document5 pagesEthics Test Bank ch3Xedis AngelNo ratings yet
- Head and Neck and Endocrine Surgery From Clinical Presentation To Treatment Success 1st Ed 2016Document400 pagesHead and Neck and Endocrine Surgery From Clinical Presentation To Treatment Success 1st Ed 2016Luan MatosNo ratings yet
- Approaches To Abdominal MassDocument49 pagesApproaches To Abdominal MassPatrick JohnNo ratings yet
- NO 4 - Airway, Breathing, Circulation, Defibrillation (April 2011) - IMSE PDFDocument3 pagesNO 4 - Airway, Breathing, Circulation, Defibrillation (April 2011) - IMSE PDFFikih Diah KusumasariNo ratings yet
- Last Exams Questions Papers 2018 Dr. Gopika PDFDocument111 pagesLast Exams Questions Papers 2018 Dr. Gopika PDFrhea100% (1)
- Ophthalmology Clinical Vignettes Oral Exam Study Guide PDFDocument41 pagesOphthalmology Clinical Vignettes Oral Exam Study Guide PDFonur temizsoylu50% (2)
- CT Scanning - Techniques and Applications PDFDocument358 pagesCT Scanning - Techniques and Applications PDFMinionNo ratings yet
- PFC - Keenan - Winter JSOM PDFDocument31 pagesPFC - Keenan - Winter JSOM PDFAlvaro PemartinNo ratings yet
- Patho PreeclampsiaDocument7 pagesPatho PreeclampsiaEliza SermoniaNo ratings yet
- Business Plan MriDocument17 pagesBusiness Plan Mriapi-298975236100% (1)
- All NCPsDocument83 pagesAll NCPsDennis Nyambane Momanyi100% (6)
- Bronchopneumonia JurnalDocument8 pagesBronchopneumonia JurnalMuhd AfizyNo ratings yet
- Tuberculosis Power PointDocument20 pagesTuberculosis Power PointLeena LapenaNo ratings yet
- (Laura Carucci) Radiologic Clinics of North Americ (BookFi) PDFDocument154 pages(Laura Carucci) Radiologic Clinics of North Americ (BookFi) PDFsebsbie admasNo ratings yet
- Fee Schedule 2010-2011Document16 pagesFee Schedule 2010-2011Chirag VaidNo ratings yet