You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- McGuffey First ReaderDocument70 pagesMcGuffey First ReaderFatma M. J. Trznadel-Skah100% (3)
- Sexual DictionaryDocument47 pagesSexual DictionaryYigit DemirelNo ratings yet
- Children's Educational Stories and Test ReviewerDocument18 pagesChildren's Educational Stories and Test ReviewerDina Dumlao88% (25)
- Simplified Tai Chi 10 FormDocument3 pagesSimplified Tai Chi 10 Formdewi_hillNo ratings yet
- Jhygfyjagfhjs DGFKUJdsghfkusd GFJKUHSDgfjhkds GFJHSDagfjhasgfjhasgdfjhgsadjfhygsdjufgvbuyjfagvbhjs DGBVJHYUSDGBVJHDSGbvjuhgvcjhsgvjhsagjhvgjhsagvjhsd GVBUKJDocument1 pageJhygfyjagfhjs DGFKUJdsghfkusd GFJKUHSDgfjhkds GFJHSDagfjhasgfjhasgdfjhgsadjfhygsdjufgvbuyjfagvbhjs DGBVJHYUSDGBVJHDSGbvjuhgvcjhsgvjhsagjhvgjhsagvjhsd GVBUKJGery RifanoNo ratings yet
- Craniotomy EVD CB Hydrocephalus Non Communicans CB IVHDocument10 pagesCraniotomy EVD CB Hydrocephalus Non Communicans CB IVHGery RifanoNo ratings yet
- Systematic ReviewDocument19 pagesSystematic ReviewGery RifanoNo ratings yet
- Daftar Stase Urologi September 2018Document1 pageDaftar Stase Urologi September 2018Gery Rifano100% (1)
- Case Report (10.00)Document11 pagesCase Report (10.00)Gery Rifano100% (1)
- Wiji 15 Juni 17Document2 pagesWiji 15 Juni 17Gery RifanoNo ratings yet
- Karakteristik Pasien Choledocholithiasis Di RSUP Dr. Kariadi Semarang Tahun 2010-2016Document4 pagesKarakteristik Pasien Choledocholithiasis Di RSUP Dr. Kariadi Semarang Tahun 2010-2016Gery RifanoNo ratings yet
- Malnutrition and Growth FailureDocument4 pagesMalnutrition and Growth FailureGery RifanoNo ratings yet
- Malignant MelanomaDocument11 pagesMalignant MelanomaGery RifanoNo ratings yet
- Cardiac TamponadeDocument10 pagesCardiac TamponadeGery RifanoNo ratings yet
- Pasien Igd Bedah Senin, 28 Agustus 2017 Dr. Jaga: AMS/ WIS/ KBN/ DK/ UDA No. CM Nama Umur/JK Diagnosa Utama Tindakan Sub Bag. KetDocument2 pagesPasien Igd Bedah Senin, 28 Agustus 2017 Dr. Jaga: AMS/ WIS/ KBN/ DK/ UDA No. CM Nama Umur/JK Diagnosa Utama Tindakan Sub Bag. KetGery RifanoNo ratings yet
- Sirosis Hepatis & Varises EsofagusDocument22 pagesSirosis Hepatis & Varises EsofagusDenata PrabhasiwiNo ratings yet
- Stase Bedah Anak Juni 2018Document1 pageStase Bedah Anak Juni 2018Gery RifanoNo ratings yet
- Complete Case-Control Study Appraisal ChecklistDocument1 pageComplete Case-Control Study Appraisal ChecklistGery RifanoNo ratings yet
- Duty Report 2-3-15Document3 pagesDuty Report 2-3-15Gery RifanoNo ratings yet
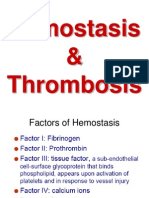
- Hemostasis & ThrombosisDocument22 pagesHemostasis & ThrombosisGery RifanoNo ratings yet
- Presentasi Parasit ResponsiDocument10 pagesPresentasi Parasit ResponsiGery RifanoNo ratings yet
- Koala PowerpointDocument9 pagesKoala Powerpointapi-237439124No ratings yet
- Actividades Aicle AnimalsDocument3 pagesActividades Aicle AnimalsMaria Jose VillarrubiaNo ratings yet
- Comedy and Tragedy in Socrates' Ideal City (CTISICDocument12 pagesComedy and Tragedy in Socrates' Ideal City (CTISICnickgrokNo ratings yet
- Atkins Diet CarbsDocument35 pagesAtkins Diet CarbsAndrei Ciobanu100% (3)
- Abdomen CavityDocument55 pagesAbdomen CavitySrisalma LasamaNo ratings yet
- Pearl Culture LectureDocument28 pagesPearl Culture LectureMahesh GKNo ratings yet
- DolphinsDocument2 pagesDolphinsdeepNo ratings yet
- Bushmen Fish PeopleDocument14 pagesBushmen Fish PeopleWesley MuhammadNo ratings yet
- Animal Farm by George Orwell Chapter 8Document13 pagesAnimal Farm by George Orwell Chapter 8TioLoloNo ratings yet
- PrincipiDocument2 pagesPrincipiSasa LeungNo ratings yet
- Echo cheat sheet guide to probe positioning viewsDocument5 pagesEcho cheat sheet guide to probe positioning viewsadelina052008No ratings yet
- Collection of business case studiesDocument2 pagesCollection of business case studiesJadiel AriasNo ratings yet
- Singapore Zoo Magazine - 201103Document19 pagesSingapore Zoo Magazine - 201103The Real Shadow ReaverNo ratings yet
- Head To Toe Assessment CompressDocument2 pagesHead To Toe Assessment CompressFitri AnnorNo ratings yet
- Short vocal warm up exercisesDocument3 pagesShort vocal warm up exercisesauroraNo ratings yet
- Coco film explores family, passion and truthDocument1 pageCoco film explores family, passion and truthFreetz TreeNo ratings yet
- 1000onethebluebo00unse 0Document142 pages1000onethebluebo00unse 0Maria MarinaNo ratings yet
- MER-KA-BA MeditationDocument10 pagesMER-KA-BA MeditationmutationxNo ratings yet
- The Kurds Thomas BoisDocument168 pagesThe Kurds Thomas BoisHoshang Salaiy100% (1)
- Po Leung Kuk 13th Primary Mathematics World Contest Team Contest 2010 questionsDocument5 pagesPo Leung Kuk 13th Primary Mathematics World Contest Team Contest 2010 questionsSanudiNo ratings yet
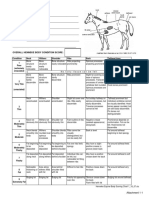
- Henneke BCS ChartDocument1 pageHenneke BCS ChartLaviniaMenicucciNo ratings yet
- The Story of Kenneth Anderson and His Wife's Bond with Sloth Bear BrunoDocument16 pagesThe Story of Kenneth Anderson and His Wife's Bond with Sloth Bear BrunoKOUSIKA S.M.No ratings yet
- Bazaar Bargains Persona Peddling Peculiar Products with ProblemsDocument10 pagesBazaar Bargains Persona Peddling Peculiar Products with ProblemsSekcerNo ratings yet
- Wolf Island: Story VocabularyDocument2 pagesWolf Island: Story VocabularyNAJLAA ALENEZINo ratings yet
- Evaluation of The Closest Speaking Space in Different Dental & Skeletal OcclusionDocument5 pagesEvaluation of The Closest Speaking Space in Different Dental & Skeletal OcclusiondrsmritiNo ratings yet
- f3 Chapter 1Document33 pagesf3 Chapter 1ROSMA287No ratings yet