You might also like
- Case 3: - Name: Mrs. M - Age: 23 Yo - Address: Lingsar, Lombok Barat - Admitted: 6 July 2017 - RM: 594222Document4 pagesCase 3: - Name: Mrs. M - Age: 23 Yo - Address: Lingsar, Lombok Barat - Admitted: 6 July 2017 - RM: 594222Ahmad HavizNo ratings yet
- Morning Report: Supervisor: Dr. Edi Prasetyo Wibowo, SP - OGDocument19 pagesMorning Report: Supervisor: Dr. Edi Prasetyo Wibowo, SP - OGGustini WidiyaningsihNo ratings yet
- Morning Report 5 April 2016 (PROM)Document64 pagesMorning Report 5 April 2016 (PROM)Brian DepamedeNo ratings yet
- Labor ReportDocument13 pagesLabor ReportSri RohmayanaNo ratings yet
- Morning Report: Supervisor: Dr. Gede Made Punarbhawa, SP - OG (K)Document13 pagesMorning Report: Supervisor: Dr. Gede Made Punarbhawa, SP - OG (K)Tannia Rizkyka IrawanNo ratings yet
- July 8, 2016: Supervisor: Dr. Juliawan SP - OG Medical Students: Ayu, Dimas, Siti ShabrinaDocument41 pagesJuly 8, 2016: Supervisor: Dr. Juliawan SP - OG Medical Students: Ayu, Dimas, Siti ShabrinaIka Putri YulianiNo ratings yet
- 04-07-12 Eklampsia PuerperiumDocument8 pages04-07-12 Eklampsia PuerperiumZainul MuttaqinNo ratings yet
- Morning Report Case of G3P2A0H2 with PROM >12 HoursDocument22 pagesMorning Report Case of G3P2A0H2 with PROM >12 HoursAhmad HavizNo ratings yet
- Morning Report 251017Document27 pagesMorning Report 251017Dewi Rabiatul AkhzamiNo ratings yet
- Morning Report August, 4 20168: Supervisor: Dr. Sp. OG DM Jaga: Verga, Hani, Nisa, SilminaDocument11 pagesMorning Report August, 4 20168: Supervisor: Dr. Sp. OG DM Jaga: Verga, Hani, Nisa, SilminaYeyen NadianNo ratings yet
- Case Report on 19-Year-Old Woman's Labor and DeliveryDocument17 pagesCase Report on 19-Year-Old Woman's Labor and DeliveryAhsanuddin Al AnsoriNo ratings yet
- MR Obgyn KPD Sabtu, 8 AprilDocument6 pagesMR Obgyn KPD Sabtu, 8 AprilRdindaaNo ratings yet
- 4 7 17 Post DateDocument11 pages4 7 17 Post DateAhmad HavizNo ratings yet
- 4 7 17 Post Date PakaiDocument8 pages4 7 17 Post Date PakaiAhmad HavizNo ratings yet
- Morning Report: Supervisor: Dr. Ario Danianto, SP - OGDocument11 pagesMorning Report: Supervisor: Dr. Ario Danianto, SP - OGGustini WidiyaningsihNo ratings yet
- Tidak Ada Pertanyaan Yang SalahDocument13 pagesTidak Ada Pertanyaan Yang SalahTannia Rizkyka IrawanNo ratings yet
- Morning Report 1 September 2014Document11 pagesMorning Report 1 September 2014Arie Krisnayanti Ida AyuNo ratings yet
- Mrs. D.S Case ReportDocument8 pagesMrs. D.S Case ReportFaishal AkbarNo ratings yet
- Jepretan Layar 2021-01-27 Pada 21.01.47Document13 pagesJepretan Layar 2021-01-27 Pada 21.01.47nadyaNo ratings yet
- MR 30 Juni 2019Document32 pagesMR 30 Juni 2019Fafan upinNo ratings yet
- Morning report from RSUD Provinsi NTBDocument17 pagesMorning report from RSUD Provinsi NTBFafan upinNo ratings yet
- Morning Report: 27 OCTOBER, 2019Document11 pagesMorning Report: 27 OCTOBER, 2019yantiNo ratings yet
- Case 3 Gemeli Breech-HeadDocument10 pagesCase 3 Gemeli Breech-Headputri laraswatiNo ratings yet
- Case I: Name: Mrs. M Age: 31 Y.O. Address:Narmada Admitted: 26 September, 2019 MR Number: 044656Document10 pagesCase I: Name: Mrs. M Age: 31 Y.O. Address:Narmada Admitted: 26 September, 2019 MR Number: 044656Inatul AuliaNo ratings yet
- Morning Report April 2nd 2016Document7 pagesMorning Report April 2nd 2016Sani Solihatul FitriNo ratings yet
- MR 22-05-2019 NewDocument8 pagesMR 22-05-2019 NewFafan upinNo ratings yet
- Severe Preeclampsia Case ReportDocument10 pagesSevere Preeclampsia Case ReportZainul MuttaqinNo ratings yet
- 11-08-2012 Kala II Kasep + CPD + SCDocument5 pages11-08-2012 Kala II Kasep + CPD + SCZainul MuttaqinNo ratings yet
- MR 18 Nov 2018 CPDDocument16 pagesMR 18 Nov 2018 CPDKuran AtikaNo ratings yet
- Morning Report: Supervisor: Dr. Windiana Rambu, SP - OGDocument12 pagesMorning Report: Supervisor: Dr. Windiana Rambu, SP - OGGustini WidiyaningsihNo ratings yet
- Morning Report: Supervisor: Dr. Made Mahayasa, SP - OGDocument5 pagesMorning Report: Supervisor: Dr. Made Mahayasa, SP - OGZainul MuttaqinNo ratings yet
- MR 23 Oktober 2019Document17 pagesMR 23 Oktober 2019yantiNo ratings yet
- MR Minus GambarDocument26 pagesMR Minus GambarmarjoranovaNo ratings yet
- Partus NormalDocument13 pagesPartus NormalGraham Allen ShowNo ratings yet
- MR 24-25 Juni 2023 Vk-Ginek-NifasDocument17 pagesMR 24-25 Juni 2023 Vk-Ginek-Nifasnining sadhaNo ratings yet
- Case Kehamilan Ektopik TergangguDocument17 pagesCase Kehamilan Ektopik TergangguwilliamNo ratings yet
- Pregnancy Induction and Gestational Hypertension AdmissionDocument18 pagesPregnancy Induction and Gestational Hypertension AdmissionKevin AgbonesNo ratings yet
- MR 24-05-2019Document12 pagesMR 24-05-2019Fafan upinNo ratings yet
- GemelliDocument4 pagesGemelliDarling Sevenfoldism SynysterNo ratings yet
- Morning Report 18 April 2016 (KPD)Document29 pagesMorning Report 18 April 2016 (KPD)ArizkamhNo ratings yet
- Morning Report 14 April 2016 (Anemia Berat)Document15 pagesMorning Report 14 April 2016 (Anemia Berat)Brian DepamedeNo ratings yet
- Partus Kasep SCDocument5 pagesPartus Kasep SCSani Solihatul FitriNo ratings yet
- Morning Report: Supervisor: Dr. Punarbawa, SP - OGDocument25 pagesMorning Report: Supervisor: Dr. Punarbawa, SP - OGRdindaaNo ratings yet
- Case ReportDocument5 pagesCase ReportSani Solihatul FitriNo ratings yet
- Morning report: Normal labor and prolonged active phase caseDocument20 pagesMorning report: Normal labor and prolonged active phase caseIka Putri YulianiNo ratings yet
- Ny. H - 34 Yo - Seteluk, Western of Sumbawa - Islam - G1P0A0L0 A/S/L/IU With Neglected 2nd Stage of LaborDocument5 pagesNy. H - 34 Yo - Seteluk, Western of Sumbawa - Islam - G1P0A0L0 A/S/L/IU With Neglected 2nd Stage of LaborZainul MuttaqinNo ratings yet
- Audit Ahad DepanDocument16 pagesAudit Ahad DepanNorfaizah FxNo ratings yet
- Morning Report: PPROM Case with HypertensionDocument29 pagesMorning Report: PPROM Case with HypertensionFeny Niifeny 'mcqueen'No ratings yet
- MR RS Unram 11 - 03 - 2021Document30 pagesMR RS Unram 11 - 03 - 2021Nia TazmaniaNo ratings yet
- Hellp 2Document57 pagesHellp 2Angela CaguitlaNo ratings yet
- (Non-Trauma) - 17 September 2023 by Ny Kusmiati (Hiscprung Disesase DD Ecrotizing Enterocolitis)Document13 pages(Non-Trauma) - 17 September 2023 by Ny Kusmiati (Hiscprung Disesase DD Ecrotizing Enterocolitis)Rasyidu MashuriNo ratings yet
- Duty Report: March 20th, 2017Document10 pagesDuty Report: March 20th, 2017Gina ArianiNo ratings yet
- MR Ny. NoniDocument5 pagesMR Ny. NoniFafan upinNo ratings yet
- HIDDENDocument12 pagesHIDDENEdvansHenryNo ratings yet
- Emergency C-Section for Pregnant Woman with EclampsiaDocument23 pagesEmergency C-Section for Pregnant Woman with Eclampsiaprimaindra27No ratings yet
- Case 2: 36 Year Old Woman with Postpartum EclampsiaDocument3 pagesCase 2: 36 Year Old Woman with Postpartum EclampsiaAinun MahtobNo ratings yet
- Advisor Dikara W.S. Maulidy:: DR., SP - PDDocument12 pagesAdvisor Dikara W.S. Maulidy:: DR., SP - PDKikiNo ratings yet
- Morning Report 12 July 2014: SPV: Dr. Edi P.W, Spog DM: Vendi, Rian, Dayu, Ayu, NurulDocument8 pagesMorning Report 12 July 2014: SPV: Dr. Edi P.W, Spog DM: Vendi, Rian, Dayu, Ayu, NurulEzraNo ratings yet
- Morning Report: Dr. Satya Leads Hospital TeamsDocument42 pagesMorning Report: Dr. Satya Leads Hospital TeamsPramudia DeniNo ratings yet
- Anemia Hemolitic X Pulmo StenosisDocument3 pagesAnemia Hemolitic X Pulmo StenosisGustini WidiyaningsihNo ratings yet
- JOURNALDocument6 pagesJOURNALGustini WidiyaningsihNo ratings yet
- Severe Anemia PDFDocument3 pagesSevere Anemia PDFGustini WidiyaningsihNo ratings yet
- Basic Concepts On Communityacquired Bacterial Pneumonia in PediatricsDocument6 pagesBasic Concepts On Communityacquired Bacterial Pneumonia in PediatricsGd Suaranta100% (1)
- Morning Report: Supervisor: Dr. Ario Danianto, SP - OGDocument11 pagesMorning Report: Supervisor: Dr. Ario Danianto, SP - OGGustini WidiyaningsihNo ratings yet
- Morning Report: Supervisor: Dr. Windiana Rambu, SP - OGDocument12 pagesMorning Report: Supervisor: Dr. Windiana Rambu, SP - OGGustini WidiyaningsihNo ratings yet
- Lung Edema PDFDocument25 pagesLung Edema PDFJoni MokodoNo ratings yet
- Managing Spontaneous Pneumothorax in a Healthy NewbornDocument2 pagesManaging Spontaneous Pneumothorax in a Healthy NewbornGustini WidiyaningsihNo ratings yet
- Retrospective Autopsy Analysis of Sepsis PatientsDocument15 pagesRetrospective Autopsy Analysis of Sepsis PatientsGustini WidiyaningsihNo ratings yet
- Spontan PneumothoraxDocument3 pagesSpontan PneumothoraxSuriyani SofianNo ratings yet
- Diagnosis and Management of Spontaneous Pneumothorax in The Emergency Department A Review of The Most Current Clinical Evidence For Diagnosis and Treatment PRRMOJ 3 127 PDFDocument7 pagesDiagnosis and Management of Spontaneous Pneumothorax in The Emergency Department A Review of The Most Current Clinical Evidence For Diagnosis and Treatment PRRMOJ 3 127 PDFGustini WidiyaningsihNo ratings yet
- Retrospective Autopsy Analysis of Sepsis PatientsDocument15 pagesRetrospective Autopsy Analysis of Sepsis PatientsGustini WidiyaningsihNo ratings yet
- Histopathological Autopsy CorrelationDocument15 pagesHistopathological Autopsy CorrelationGustini WidiyaningsihNo ratings yet
- Exercises - Nominal and Relative ClausesDocument23 pagesExercises - Nominal and Relative ClausesRoxana ȘtefanNo ratings yet
- Chem237LabManual Fall2012 RDocument94 pagesChem237LabManual Fall2012 RKyle Tosh0% (1)
- Tema 14Document6 pagesTema 14LaiaNo ratings yet
- Portfolio FormatDocument7 pagesPortfolio Formatcelestine fordNo ratings yet
- Top 25 Likely Project Defense Questions and AnswersDocument18 pagesTop 25 Likely Project Defense Questions and AnswersCathrina Therese P. CornitaNo ratings yet
- Goal Setting - FinalDocument2 pagesGoal Setting - Finalapi-301796386No ratings yet
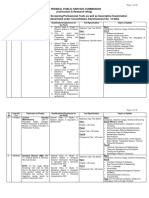
- FEDERAL PUBLIC SERVICE COMMISSION SCREENING/PROFESSIONAL TESTSDocument36 pagesFEDERAL PUBLIC SERVICE COMMISSION SCREENING/PROFESSIONAL TESTSCh Hassan TajNo ratings yet
- Beg U11 Revision PDFDocument2 pagesBeg U11 Revision PDFBonny IvoNo ratings yet
- 5 Teacher Work Sample Final - BeckhamDocument39 pages5 Teacher Work Sample Final - Beckhamapi-720960934No ratings yet
- 1st Grade PYP Planner Unit 3Document4 pages1st Grade PYP Planner Unit 3Irish CortezNo ratings yet
- Trigonometric Ratios: Find The Value of Each Trigonometric RatioDocument2 pagesTrigonometric Ratios: Find The Value of Each Trigonometric RatioRandom EmailNo ratings yet
- RPP Struktur AtomDocument4 pagesRPP Struktur AtomFawnia D'Genkbellzz Ezzar FluorinAnindyaNo ratings yet
- Diversity in The Workplace: Industrial-Organizational Psychology Learning ModuleDocument10 pagesDiversity in The Workplace: Industrial-Organizational Psychology Learning ModuleVukashin.meNo ratings yet
- DepEd issues guidelines for ALS presentation portfolio assessmentDocument27 pagesDepEd issues guidelines for ALS presentation portfolio assessmentJessica MataNo ratings yet
- Weekly Report, Literature Meeting 2Document2 pagesWeekly Report, Literature Meeting 2Suzy NadiaNo ratings yet
- IT1 ReportDocument1 pageIT1 ReportFranz Allen RanasNo ratings yet
- List of Participants: Name Institution Country E-MailDocument5 pagesList of Participants: Name Institution Country E-MailFrancis MorrisonNo ratings yet
- Shabnam Mehrtash, Settar Koçak, Irmak Hürmeriç Altunsöz: Hurmeric@metu - Edu.trDocument11 pagesShabnam Mehrtash, Settar Koçak, Irmak Hürmeriç Altunsöz: Hurmeric@metu - Edu.trsujiNo ratings yet
- A Comparative Study of Volleyball Skill Between National and College Level Player Through Volleyball TestDocument56 pagesA Comparative Study of Volleyball Skill Between National and College Level Player Through Volleyball TestMullah 302No ratings yet
- Practical Research 2 Quarter 4 Module 5 Lesson 1Document2 pagesPractical Research 2 Quarter 4 Module 5 Lesson 1juvy abelleraNo ratings yet
- Newsletter 3.1Document12 pagesNewsletter 3.1mrifenburgNo ratings yet
- The Id, Ego and The Superego - Sigmund FreudDocument6 pagesThe Id, Ego and The Superego - Sigmund FreudsiddhantkhandelwalNo ratings yet
- Undertaking Cum Indemnity BondDocument3 pagesUndertaking Cum Indemnity BondActs N FactsNo ratings yet
- SHRM PPT Chap 4Document29 pagesSHRM PPT Chap 4Jamshed AhmedNo ratings yet
- Study Skills For SpellingDocument2 pagesStudy Skills For Spellingapi-277816141No ratings yet
- An Analysis of Extrinsic Elements in The Freedom Writers MovieDocument3 pagesAn Analysis of Extrinsic Elements in The Freedom Writers MovieNinda AlfiaNo ratings yet
- Understand SWOT Analysis in 40 CharactersDocument6 pagesUnderstand SWOT Analysis in 40 Characterstapan mistryNo ratings yet
- Grade 11 Math Lesson Log on FunctionsDocument4 pagesGrade 11 Math Lesson Log on FunctionsMardy Nelle Sanchez Villacura-Galve100% (2)
- Manual Lymph DrainageDocument6 pagesManual Lymph DrainageArdelean Dragos100% (1)
- Mother Tongue Lesson Week 7Document7 pagesMother Tongue Lesson Week 7ElsieJhadeWandasAmandoNo ratings yet