You might also like
- ATLS PretestDocument133 pagesATLS Pretestmarcelina100% (1)
- Jurnal Psikologi Indonesia Vol 6 No 1 20Document84 pagesJurnal Psikologi Indonesia Vol 6 No 1 20marcelinaNo ratings yet
- New Treatment Options For Metastatic Thyroid CancerDocument6 pagesNew Treatment Options For Metastatic Thyroid CancermarcelinaNo ratings yet
- Influence of work ethic & organizational culture on teacher professionalismDocument17 pagesInfluence of work ethic & organizational culture on teacher professionalismNelil MunaNo ratings yet
- Internasional Jurnal Pendidikan PDFDocument284 pagesInternasional Jurnal Pendidikan PDFjurnalNo ratings yet
- Jurnal Internasional - Katsesart JurnalDocument8 pagesJurnal Internasional - Katsesart JurnalmarcelinaNo ratings yet
- Pediatric Disease PresentationDocument47 pagesPediatric Disease PresentationUrinaria Kel 6No ratings yet
- (PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFDocument157 pages(PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFmarcelinaNo ratings yet
- Pustaka Unpad Tatalaksana - Penyakit - JantungDocument44 pagesPustaka Unpad Tatalaksana - Penyakit - JantungmarcelinaNo ratings yet
- Acute HF Slides 2005Document55 pagesAcute HF Slides 2005Ayu Puspita SariNo ratings yet
- Pediatric Disease PresentationDocument47 pagesPediatric Disease PresentationUrinaria Kel 6No ratings yet
- Diagnosis and Management of Cyanotic Congenital HeDocument15 pagesDiagnosis and Management of Cyanotic Congenital HemarcelinaNo ratings yet
- Pcos-Guideline Master 05022018 7-1Document185 pagesPcos-Guideline Master 05022018 7-1Lotfy LotfyNo ratings yet
- Associate Clinical Prof. Dr. Aisha M. El-Bareg, MD, PHD Senior Consultant in (Obs & Gyn) /reproductive Medicine Faculty of Medicine, Misurata University, LibyaDocument18 pagesAssociate Clinical Prof. Dr. Aisha M. El-Bareg, MD, PHD Senior Consultant in (Obs & Gyn) /reproductive Medicine Faculty of Medicine, Misurata University, LibyamarcelinaNo ratings yet
- 10 1016@j Jpeds 2017 11 065Document10 pages10 1016@j Jpeds 2017 11 065Anonymous OjlR4HLNo ratings yet
- Why Propranolol Is Preferred To Other BetaDocument3 pagesWhy Propranolol Is Preferred To Other BetamarcelinaNo ratings yet
- Yang 2017Document6 pagesYang 2017marcelinaNo ratings yet
- Diagnosis and Management of Tonsillitis GuidelineDocument23 pagesDiagnosis and Management of Tonsillitis GuidelinemarcelinaNo ratings yet
- Acute suppurative parotitis in early infancyDocument2 pagesAcute suppurative parotitis in early infancymarcelinaNo ratings yet
- Anti Angina (Hany)Document51 pagesAnti Angina (Hany)marcelinaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nursing Management of a Patient with Kawasaki DiseaseDocument49 pagesNursing Management of a Patient with Kawasaki DiseaseJemimah Ruth Madayag ValenzuelaNo ratings yet
- Angina/Non-ST-elevation Myocardial Infarction: B-Type Natriuretic Peptide Evaluation of B-Type Natriuretic Peptide For Risk Assessment in UnstableDocument12 pagesAngina/Non-ST-elevation Myocardial Infarction: B-Type Natriuretic Peptide Evaluation of B-Type Natriuretic Peptide For Risk Assessment in Unstablesyaiful rinantoNo ratings yet
- The Circulatory System Stations - Sbi3uDocument3 pagesThe Circulatory System Stations - Sbi3uapi-394529729No ratings yet
- Cardiovascular System OverviewDocument122 pagesCardiovascular System OverviewAdrian Rosell Carrillo EnriquezNo ratings yet
- Rekapitulasi Kunjungan Pasien BPJS: NO Tanggal No Kartu Nama PesertaDocument30 pagesRekapitulasi Kunjungan Pasien BPJS: NO Tanggal No Kartu Nama PesertaEdo Anugrah HutamaNo ratings yet
- Improvements in Cardiac Patients Through Exercise TrainingDocument41 pagesImprovements in Cardiac Patients Through Exercise Trainingifan zulfantriNo ratings yet
- Intracranial Brain TumorDocument24 pagesIntracranial Brain TumorheruNo ratings yet
- Cardiac Case StudyDocument3 pagesCardiac Case Studydsaitta108No ratings yet
- Mathematical Model On Cardiovascular and Respiratory System Modelling Seminar ReportDocument50 pagesMathematical Model On Cardiovascular and Respiratory System Modelling Seminar ReportfelipeNo ratings yet
- CABGDocument17 pagesCABGpnanees100% (1)
- AnticoagulantsDocument26 pagesAnticoagulantsimnnayakNo ratings yet
- Noradrenaline Guide for Neonatal Shock & Pulmonary HypertensionDocument3 pagesNoradrenaline Guide for Neonatal Shock & Pulmonary HypertensionArif212 ArifNo ratings yet
- 2 - Holter ECG - TLC5000 Dynamic ECG SystemDocument3 pages2 - Holter ECG - TLC5000 Dynamic ECG SystemChristian Donfack fogang100% (1)
- St. Paul School Science Exam PrepDocument3 pagesSt. Paul School Science Exam PrepIrish Jhaizel Kaye FuentesNo ratings yet
- Lesson9 Cardiovascular AssessmentDocument21 pagesLesson9 Cardiovascular AssessmentDennis Nabor Muñoz, RN,RMNo ratings yet
- Varicose Vein - Management, DVT: BY Anandhu Lal Anjali P K AnjusjDocument108 pagesVaricose Vein - Management, DVT: BY Anandhu Lal Anjali P K AnjusjAsif AbbasNo ratings yet
- Resuscitation: ILCOR Summary StatementDocument13 pagesResuscitation: ILCOR Summary StatementLuis-alfredo Perez Bolde HernandezNo ratings yet
- Antithrombotic Therapy After Revascularization in Patients With Peripheral Arterial Disease: What Is Here, What Is NextDocument12 pagesAntithrombotic Therapy After Revascularization in Patients With Peripheral Arterial Disease: What Is Here, What Is NextenviNo ratings yet
- Valvularheart Diseases: PathophysiologyDocument9 pagesValvularheart Diseases: PathophysiologyVoid LessNo ratings yet
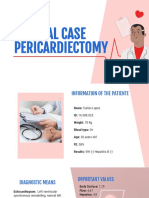
- Clinical Case 1 PericardiectomyDocument11 pagesClinical Case 1 Pericardiectomyapi-654112138No ratings yet
- Upper Extremity Venous Protocol 14Document2 pagesUpper Extremity Venous Protocol 14api-349402240No ratings yet
- Inp PathoDocument1 pageInp PathoNoveeNo ratings yet
- Abstract IctromiDocument2 pagesAbstract Ictromiyayasan harapan ummatNo ratings yet
- Knowledge and behavior of acute coronary syndrome patientsDocument10 pagesKnowledge and behavior of acute coronary syndrome patientsFATIMAH WANDANo ratings yet
- Histology of The Cardiovascular System-3Document54 pagesHistology of The Cardiovascular System-3lessank12No ratings yet
- Cardiovascular NotesDocument18 pagesCardiovascular NotesCathy SantosNo ratings yet
- Left Bundle Branch BlockDocument10 pagesLeft Bundle Branch BlockMochamad BasriNo ratings yet
- WP Contentuploads201805CABANA Trial Slides 05092018FINAL PDFDocument19 pagesWP Contentuploads201805CABANA Trial Slides 05092018FINAL PDFJjawo GinesNo ratings yet
- Ebook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFDocument40 pagesEbook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFalexandercampbelldkcnzafgtw100% (9)
- Blood Clots: How Does Blood Clot?Document2 pagesBlood Clots: How Does Blood Clot?Pebrian Diki PrestyaNo ratings yet