You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Sept 2020 MRCS RecallsDocument46 pagesSept 2020 MRCS RecallsGiovanni Henry75% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Tracheal StenosisDocument5 pagesTracheal StenosisGiovanni HenryNo ratings yet
- September 2020 Recalls Scorpio and Al Beruni 243 QuestionsDocument9 pagesSeptember 2020 Recalls Scorpio and Al Beruni 243 QuestionsGiovanni HenryNo ratings yet
- Anterior Pharyngeal PouchDocument4 pagesAnterior Pharyngeal PouchGiovanni HenryNo ratings yet
- Reirradiation Meta Analysis and Systematic ReviewDocument13 pagesReirradiation Meta Analysis and Systematic ReviewGiovanni HenryNo ratings yet
- Medical EMQs and Clinical ScenariosDocument18 pagesMedical EMQs and Clinical ScenariosMehdi Hasan MazumderNo ratings yet
- Defining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranDocument104 pagesDefining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranGiovanni HenryNo ratings yet
- Endoscopic Sinus SurgeryDocument91 pagesEndoscopic Sinus SurgeryGiovanni HenryNo ratings yet
- Paediatric Neck MassesDocument7 pagesPaediatric Neck MassesGiovanni HenryNo ratings yet
- Evaluation of The Dizzy PatientDocument61 pagesEvaluation of The Dizzy PatientGiovanni HenryNo ratings yet
- Defining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranDocument104 pagesDefining Physiology: Principles, Themes, Concepts.: Hwee Ming Cheng Kin Kheong Mah Kumar SeluakumaranGiovanni HenryNo ratings yet
- April 2018 Recalls - Reda: Embolectomy??)Document5 pagesApril 2018 Recalls - Reda: Embolectomy??)Giovanni HenryNo ratings yet
- Clinical Features of Ramsay Hunt Syndrome.: C J Sweeney, and D H Gilden J Neurol Neurosurg Psychiatry 2001 71:149-154Document1 pageClinical Features of Ramsay Hunt Syndrome.: C J Sweeney, and D H Gilden J Neurol Neurosurg Psychiatry 2001 71:149-154Giovanni HenryNo ratings yet
- 2018 Cardiovascular PhysiologyDocument197 pages2018 Cardiovascular PhysiologyGladys ParedesNo ratings yet
- Recalls of Paper 2 - 11/9/2018: ConsentDocument6 pagesRecalls of Paper 2 - 11/9/2018: ConsentGiovanni Henry0% (1)
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- April 2018 IMRCS A Exam ReviewDocument12 pagesApril 2018 IMRCS A Exam Reviewmobz00No ratings yet
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- General Surgery June 2010: Paper IDocument2 pagesGeneral Surgery June 2010: Paper IGiovanni HenryNo ratings yet
- Endothelium I: Atherogenesis: Maintenance of Vascular HomeostasisDocument5 pagesEndothelium I: Atherogenesis: Maintenance of Vascular HomeostasisGiovanni HenryNo ratings yet
- Transplantation: Leo-Paul Powell DM Tutorial Series March 30, 2021Document45 pagesTransplantation: Leo-Paul Powell DM Tutorial Series March 30, 2021Giovanni HenryNo ratings yet
- Surgical AnatomyDocument4 pagesSurgical AnatomyGiovanni HenryNo ratings yet
- Gen Surg 1996 2009Document26 pagesGen Surg 1996 2009LijoeliyasNo ratings yet
- The Physiology of Human DefecationDocument21 pagesThe Physiology of Human Defecationyohanna yohannaNo ratings yet
- Surgery Questions EssayDocument11 pagesSurgery Questions Essaymimycutey100% (3)
- EVAR vs. Open Repair - EvidenceDocument5 pagesEVAR vs. Open Repair - EvidenceGiovanni HenryNo ratings yet
- Frcs Viva TOPICSDocument4 pagesFrcs Viva TOPICSGiovanni HenryNo ratings yet
- Colon & Rectum Questions Aug 2008Document61 pagesColon & Rectum Questions Aug 2008Dr.mesho Bin MansourNo ratings yet
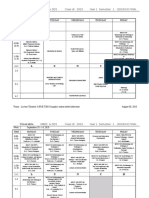
- Class of 2023 Year 1 Sem 1 Final Aug 30Document16 pagesClass of 2023 Year 1 Sem 1 Final Aug 30Giovanni HenryNo ratings yet
- Kelly's Panel Hospital: Hospital Name Address Tel No Kuala LumpurDocument9 pagesKelly's Panel Hospital: Hospital Name Address Tel No Kuala LumpurSEAN LAINo ratings yet
- THESIS (Depression)Document13 pagesTHESIS (Depression)Kimberly NgNo ratings yet
- Eudaimonia in The Contemporary Science of Subjective Well-Being - Psychological Well-Being, Self-Determination, and Meaning in LifeDocument14 pagesEudaimonia in The Contemporary Science of Subjective Well-Being - Psychological Well-Being, Self-Determination, and Meaning in LifeAlvin CsunderlikNo ratings yet
- Module 5 Southeastern and Northeastern DanceDocument10 pagesModule 5 Southeastern and Northeastern DanceJoner L. GIRAONo ratings yet
- Evaluation of Toxicity of Synthetic Food Colors On Human Normal Flora and YeastDocument5 pagesEvaluation of Toxicity of Synthetic Food Colors On Human Normal Flora and YeastSonali KalitaNo ratings yet
- How to Cite Patient Safety Incident Reporting SystemDocument7 pagesHow to Cite Patient Safety Incident Reporting System'Amel'AyuRizkyAmeliyahNo ratings yet
- The Concept of Intersubjectivity - BohleberDocument19 pagesThe Concept of Intersubjectivity - BohleberJanina BarbuNo ratings yet
- ThunderBay Event RevisedDocument1 pageThunderBay Event RevisedLyane ZygmuntNo ratings yet
- Activity-Based Implementation and Evaluation Plan Summary (Used As SETT Scaffold For Implementation and Evaluation Planning)Document1 pageActivity-Based Implementation and Evaluation Plan Summary (Used As SETT Scaffold For Implementation and Evaluation Planning)api-289181874No ratings yet
- Hazbin Hotel OC Frank (Update)Document2 pagesHazbin Hotel OC Frank (Update)Francisco Jose Nieto GarciaNo ratings yet
- Pilot II: Technical Data SheetDocument4 pagesPilot II: Technical Data SheetSafinahNo ratings yet
- Hunting VocabularyDocument1 pageHunting Vocabularygermanvip8No ratings yet
- Transcultural Nursing Theories - Leininger and OremDocument22 pagesTranscultural Nursing Theories - Leininger and OremArah Lyn ApiagNo ratings yet
- Paranoid SNDocument3 pagesParanoid SNmalindaNo ratings yet
- Tinywow - 2 - Atellica - CH - Assay - Overview - 51352597Document16 pagesTinywow - 2 - Atellica - CH - Assay - Overview - 51352597sohba2000No ratings yet
- Title of Paper (Font Times New Roman, 12 PT, 1 Space, Centered)Document3 pagesTitle of Paper (Font Times New Roman, 12 PT, 1 Space, Centered)farikoNo ratings yet
- Model CVDocument4 pagesModel CVDany SimaNo ratings yet
- NEBOSH HSE Certification in Health and Safety Leadership ExcellenceDocument18 pagesNEBOSH HSE Certification in Health and Safety Leadership ExcellenceRahul Siwakoti100% (1)
- The School Canteen Follows Guidelines On Operational Management Set by The Department of Education Through DepEd Order NoDocument3 pagesThe School Canteen Follows Guidelines On Operational Management Set by The Department of Education Through DepEd Order NoChristian Lloyd Latayan64% (14)
- Table 5-8 - DSM-5 Diagnostic Criteria For Panic DisorderDocument1 pageTable 5-8 - DSM-5 Diagnostic Criteria For Panic DisorderDragutin PetrićNo ratings yet
- Challenge 6.0 Gym CutDocument38 pagesChallenge 6.0 Gym CutBurcu SenolNo ratings yet
- Task 2 Case Notes: James Hutton: Time AllowedDocument3 pagesTask 2 Case Notes: James Hutton: Time AllowedKelvin Kanengoni0% (1)
- ConstructivismDocument16 pagesConstructivismKhoiruddin Bashori50% (2)
- Treatment of HypertensionDocument23 pagesTreatment of HypertensionRABIATUL ADAWIYAHNo ratings yet
- White Mineral Oil SDSDocument4 pagesWhite Mineral Oil SDSAreIf Cron BmxStreetNo ratings yet
- Ic5 HD Ral - Ifu - X4054 en 13 - 20200323Document64 pagesIc5 HD Ral - Ifu - X4054 en 13 - 20200323Abdul HamidNo ratings yet
- Male, Masculinities Methodologies and MethodsDocument40 pagesMale, Masculinities Methodologies and MethodsMarco Rojas VNo ratings yet
- Acl Reconstruction Without Meniscus RepairDocument1 pageAcl Reconstruction Without Meniscus Repairsathvik gowdaNo ratings yet
- Spilling The Tea Culture Report by - KommuneDocument88 pagesSpilling The Tea Culture Report by - KommuneSmriti TewariNo ratings yet
- Stress Eating: A Phenomenological StudyDocument24 pagesStress Eating: A Phenomenological StudyGauis Laurence CaraoaNo ratings yet