You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Acrrm Recalls Latest PDFDocument16 pagesAcrrm Recalls Latest PDFRumana Ali100% (2)
- When Not To Stop A Clinical Trial.23490736Document4 pagesWhen Not To Stop A Clinical Trial.23490736Gloria KartikaNo ratings yet
- Survival Analysis, Part 3: Cox Regression: Statistics and Research DesignDocument2 pagesSurvival Analysis, Part 3: Cox Regression: Statistics and Research DesignGloria KartikaNo ratings yet
- Prevalensi Ventricular HypertrophyDocument8 pagesPrevalensi Ventricular HypertrophyGloria KartikaNo ratings yet
- 24 Newsletter Hypertension and ArrhythmiaDocument2 pages24 Newsletter Hypertension and ArrhythmiaGloria KartikaNo ratings yet
- Contoh Surat SponsorDocument1 pageContoh Surat SponsorGloria KartikaNo ratings yet
- QTinterval Changes During The Management of DHFDocument7 pagesQTinterval Changes During The Management of DHFGloria KartikaNo ratings yet
- MC GowanDocument13 pagesMC GowanGloria KartikaNo ratings yet
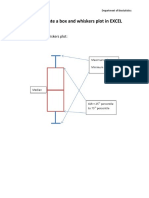
- How To Create A Box and Whiskers Plot in EXCELDocument9 pagesHow To Create A Box and Whiskers Plot in EXCELGloria KartikaNo ratings yet
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDocument4 pagesInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaNo ratings yet
- Cardiology Board Review - Carlquist - PT. 1 PDFDocument40 pagesCardiology Board Review - Carlquist - PT. 1 PDFGloria KartikaNo ratings yet
- WHO LadderDocument2 pagesWHO LaddertelorkodokNo ratings yet
- CLN 66 01 107 PDFDocument5 pagesCLN 66 01 107 PDFGloria KartikaNo ratings yet
- WHO Blindness Action An 2014-2019Document28 pagesWHO Blindness Action An 2014-2019Gloria KartikaNo ratings yet
- Vision2020 ReportDocument97 pagesVision2020 ReportAdelaida Castro NavarreteNo ratings yet
- Degeneratif Copy 2Document7 pagesDegeneratif Copy 2Gloria KartikaNo ratings yet
- Clinical Management 07Document22 pagesClinical Management 07Fauzi SatriaNo ratings yet
- WHO Clinical Management 0f Avian InfluenzaDocument83 pagesWHO Clinical Management 0f Avian InfluenzaGloria KartikaNo ratings yet
- Infeksi Marginalis NadaDocument48 pagesInfeksi Marginalis NadaGloria KartikaNo ratings yet
- Staining and Tooth DiscolorationDocument14 pagesStaining and Tooth DiscolorationGloria KartikaNo ratings yet
- CH 06Document11 pagesCH 06kavitasibalNo ratings yet
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- Hypertension: H.) or May Be Associated With Other Diseases - Dorland'sDocument1 pageHypertension: H.) or May Be Associated With Other Diseases - Dorland'sGloria KartikaNo ratings yet
- Assessment of Using Guava Leaves As An Alternative Medicine For DiarrheaDocument32 pagesAssessment of Using Guava Leaves As An Alternative Medicine For DiarrheaKamela AliNo ratings yet
- Gabriel Ogun StateDocument15 pagesGabriel Ogun Statedavid ojNo ratings yet
- Nausea and Vomiting, The Basics: DefinitionsDocument2 pagesNausea and Vomiting, The Basics: DefinitionsNoobNo ratings yet
- ENGLISH 6 - Q1 - W5 - Mod5 - Make Connection Between Information ViewDocument15 pagesENGLISH 6 - Q1 - W5 - Mod5 - Make Connection Between Information Viewerma rose hernandezNo ratings yet
- JSA - Doc Job Safety Analysis NewDocument3 pagesJSA - Doc Job Safety Analysis NewKali MuthuNo ratings yet
- Sample Synthesis Essay - DepressionDocument3 pagesSample Synthesis Essay - DepressionKaren ReasonNo ratings yet
- AUBF QUiZDocument12 pagesAUBF QUiZGene Narune GaronitaNo ratings yet
- Students With Mental RetardationDocument3 pagesStudents With Mental RetardationNorain KasanNo ratings yet
- Pelargonium SidoidesDocument2 pagesPelargonium SidoidesceramickurtNo ratings yet
- Mental Health Effects of ObesityDocument7 pagesMental Health Effects of ObesityMohd FaizNo ratings yet
- ChromagarDocument2 pagesChromagarapi-26429188No ratings yet
- CVJ anatomy classification and clinical signsDocument53 pagesCVJ anatomy classification and clinical signssa2tigNo ratings yet
- IMCIDocument11 pagesIMCIJoshua Villarba100% (1)
- TofacitinibDocument23 pagesTofacitinibShubham SenguptaNo ratings yet
- Lab Values Cheat SheetDocument3 pagesLab Values Cheat Sheetmadison61404No ratings yet
- National Institute On Aging Publications CatalogDocument32 pagesNational Institute On Aging Publications CatalogAbex ComprasNo ratings yet
- Subject Sub-Subject Topic NameDocument6 pagesSubject Sub-Subject Topic NameHemanth Manikanta Sai PosaNo ratings yet
- Payment Policies and Agreement To PayDocument5 pagesPayment Policies and Agreement To PayChristopher HartmanNo ratings yet
- Health and Safety at Work in Europe STATISTICS EUROSTAT 2010 PDFDocument103 pagesHealth and Safety at Work in Europe STATISTICS EUROSTAT 2010 PDFAmer H DobrachaNo ratings yet
- One Point Acupressure Treatment AllDocument23 pagesOne Point Acupressure Treatment AllPraveen Kumar100% (1)
- Drug laxative reduces ammonia lactuloseDocument6 pagesDrug laxative reduces ammonia lactuloseRj MagalingNo ratings yet
- Emergency Room Care Plan for HyperthermiaDocument7 pagesEmergency Room Care Plan for HyperthermiaNatasha Alaine E. CayabyabNo ratings yet
- Notes On History Taking in The Cardiovascular SystemDocument9 pagesNotes On History Taking in The Cardiovascular Systemmdjohar72100% (1)
- Thyroid Disease Anesthetic ConsiderationsDocument30 pagesThyroid Disease Anesthetic Considerationssachin10dulkarNo ratings yet
- Fixed Drug EruptionsDocument6 pagesFixed Drug EruptionsArif OktavianNo ratings yet
- Remember This - FoerDocument2 pagesRemember This - FoerElham AhmedNo ratings yet
- Simple Indigestion in RuminantsDocument11 pagesSimple Indigestion in RuminantsAli H. Sadiek أ.د. علي حسن صديق75% (4)
- FSH and LH LevelsDocument4 pagesFSH and LH Levelsujjwal guptaNo ratings yet